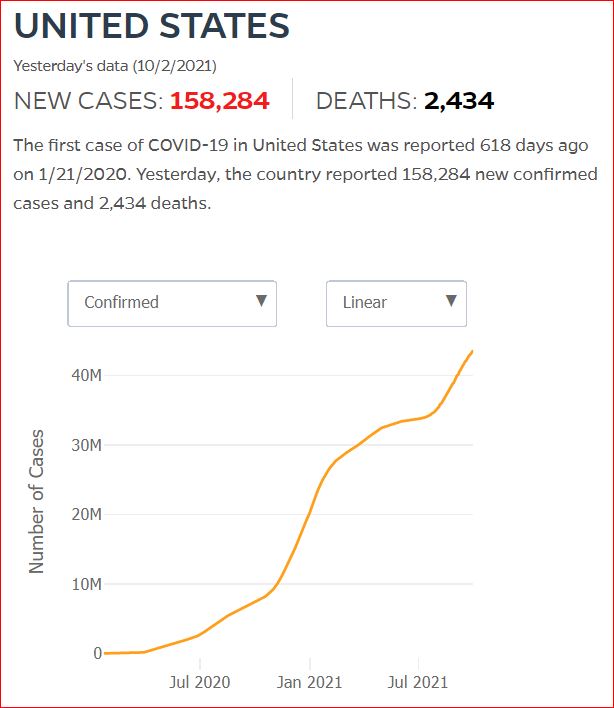
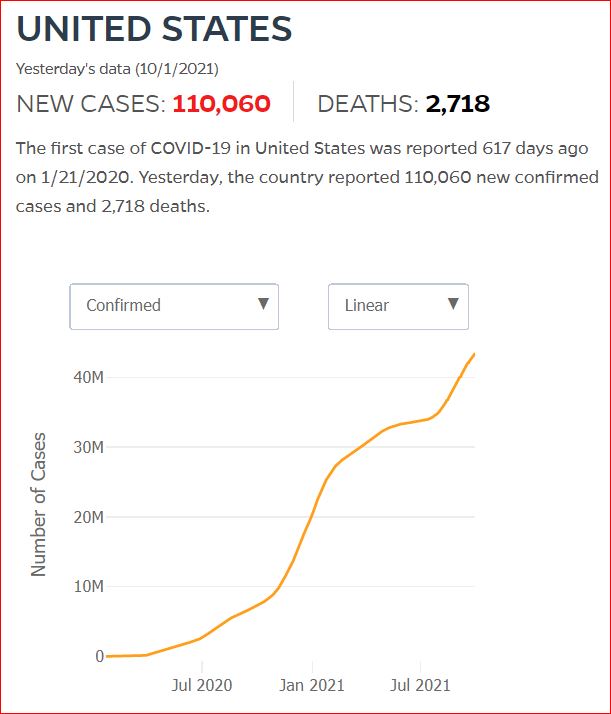
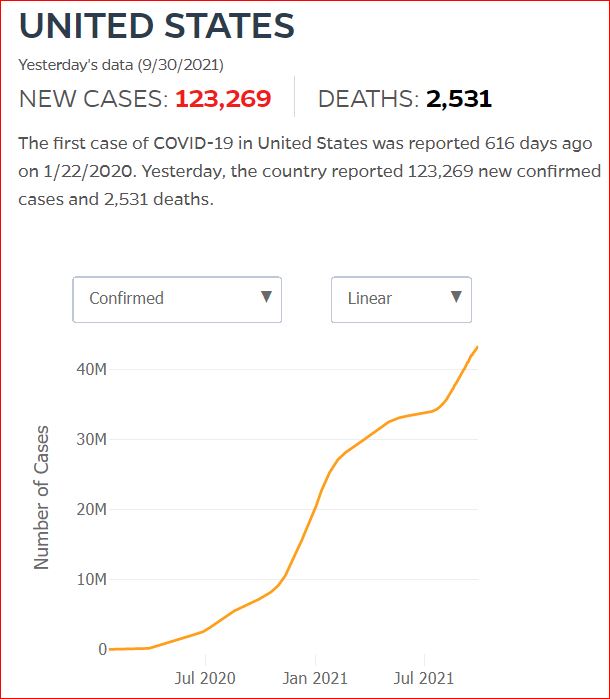
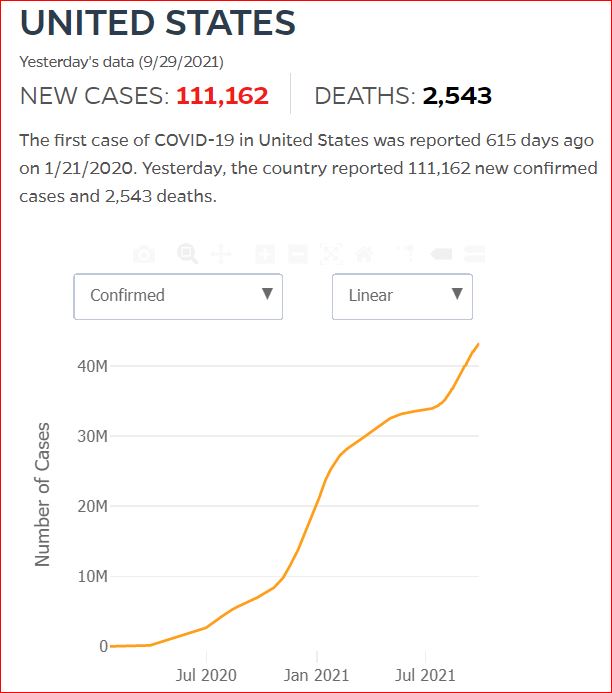
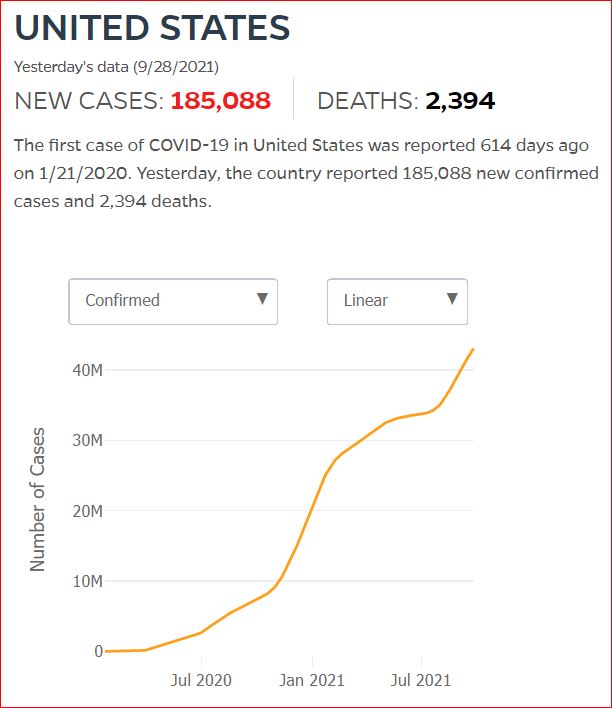


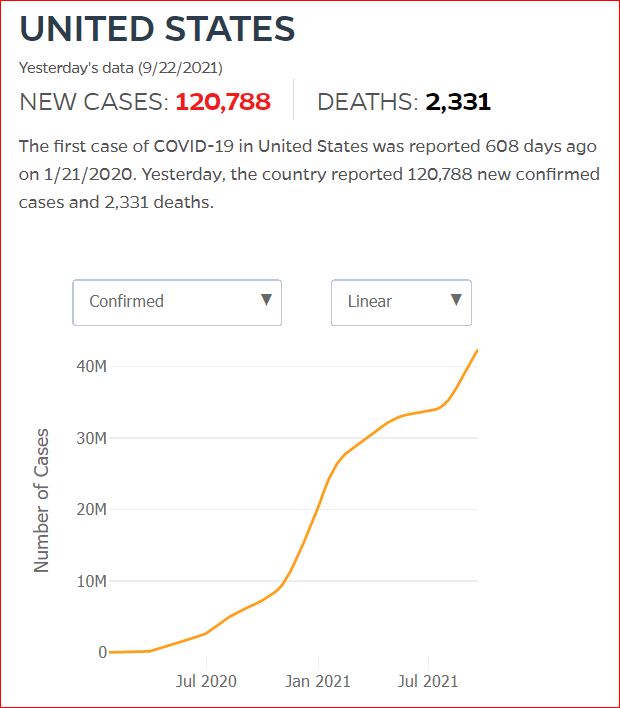



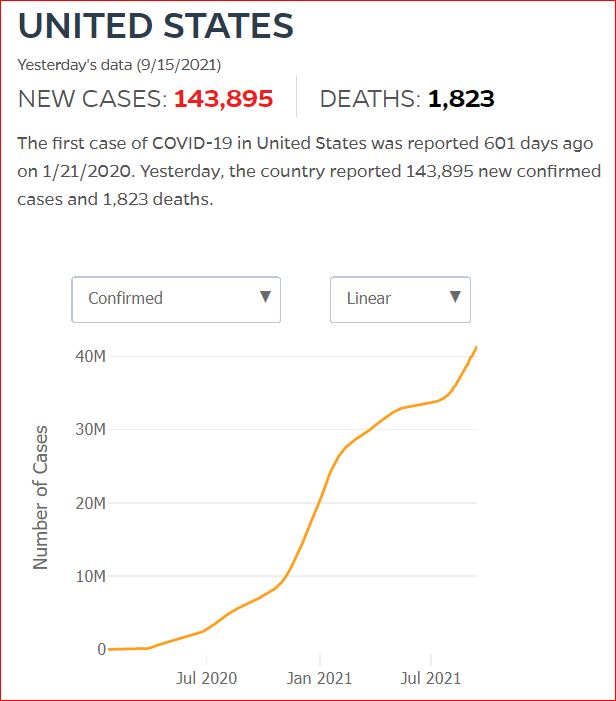

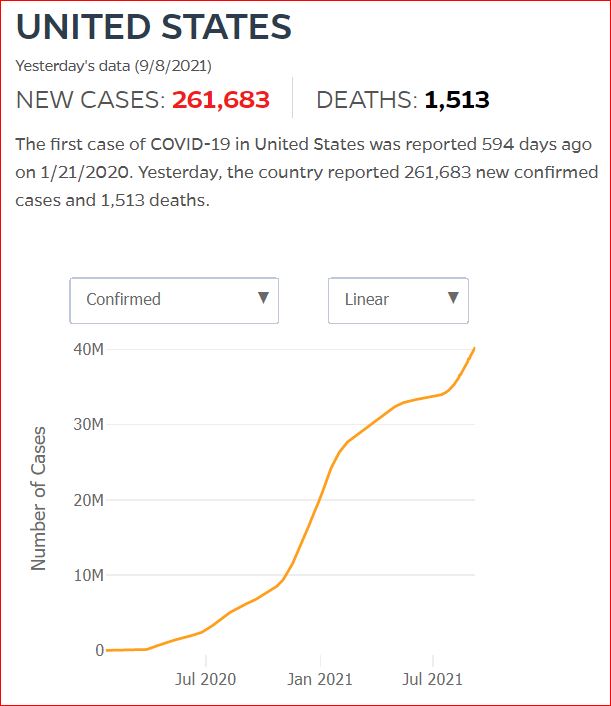
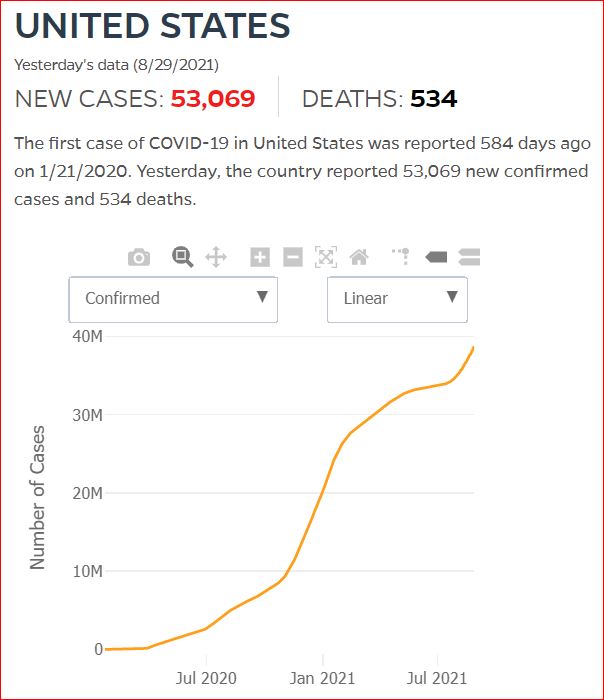
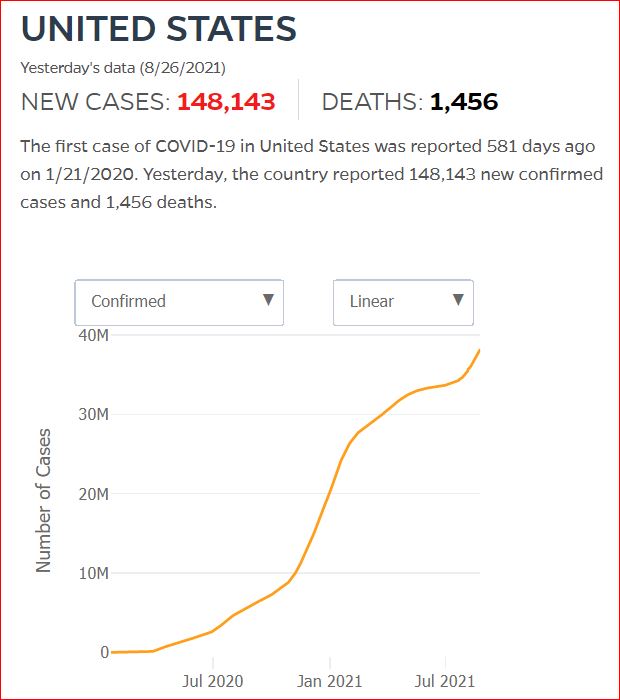
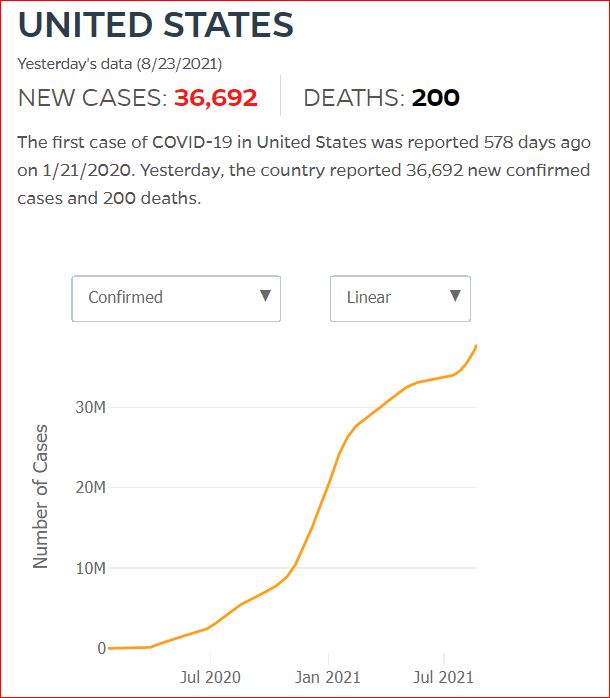
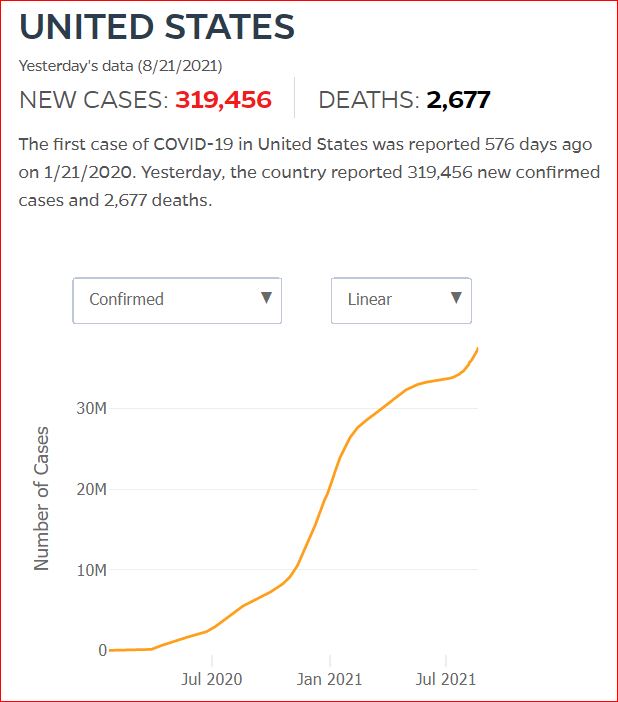
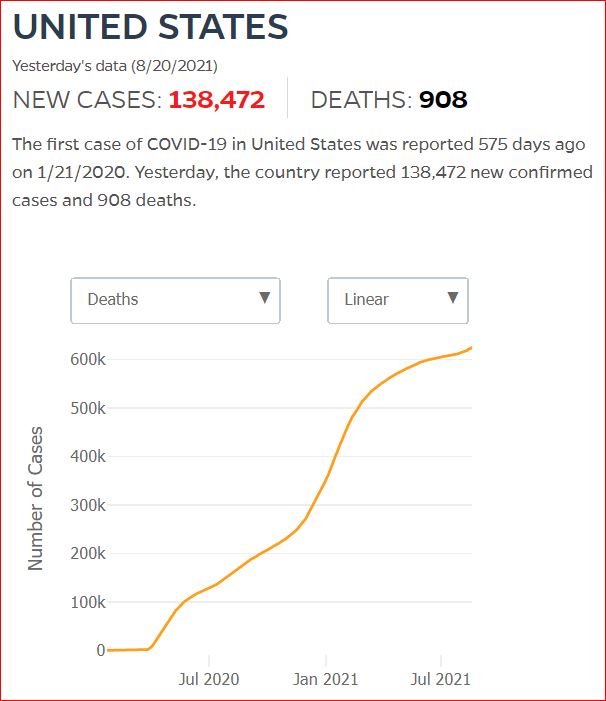
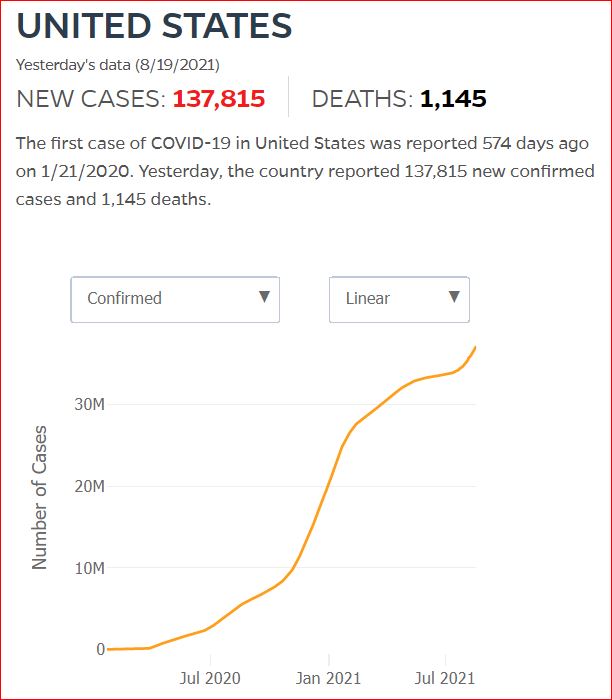
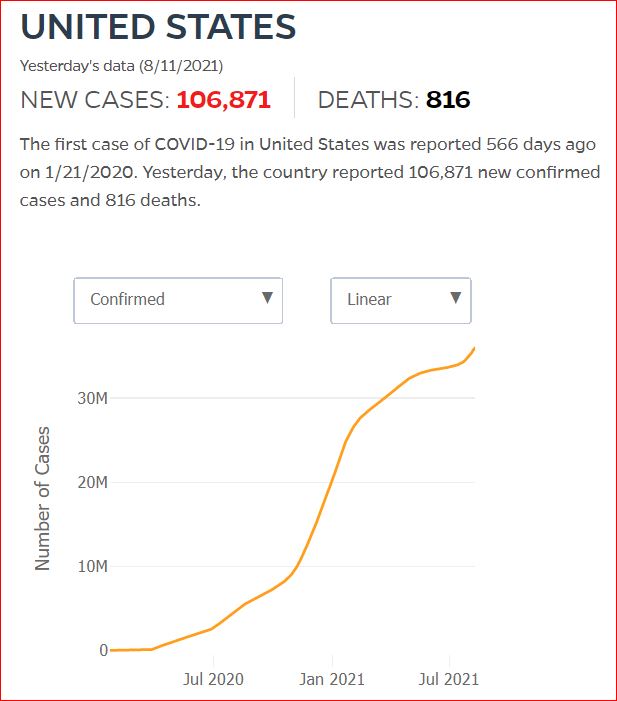
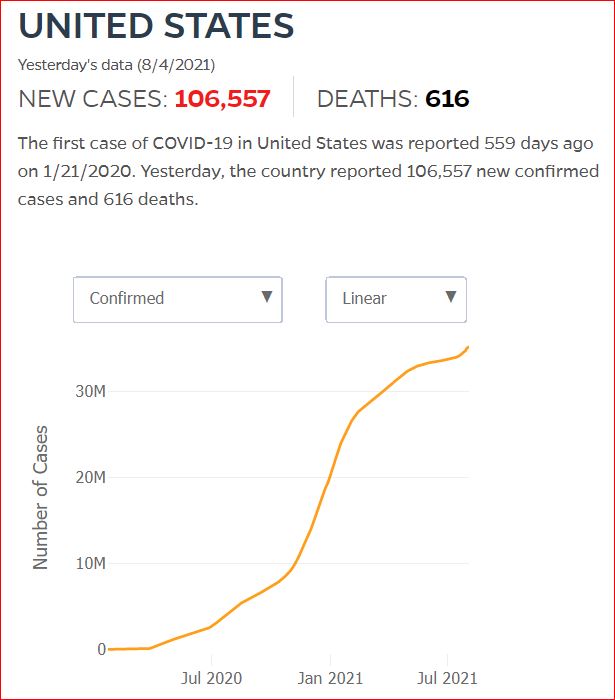
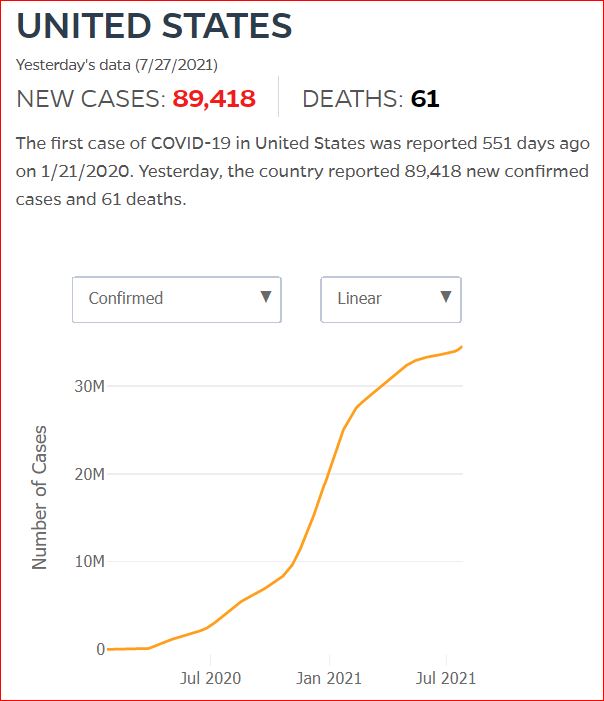
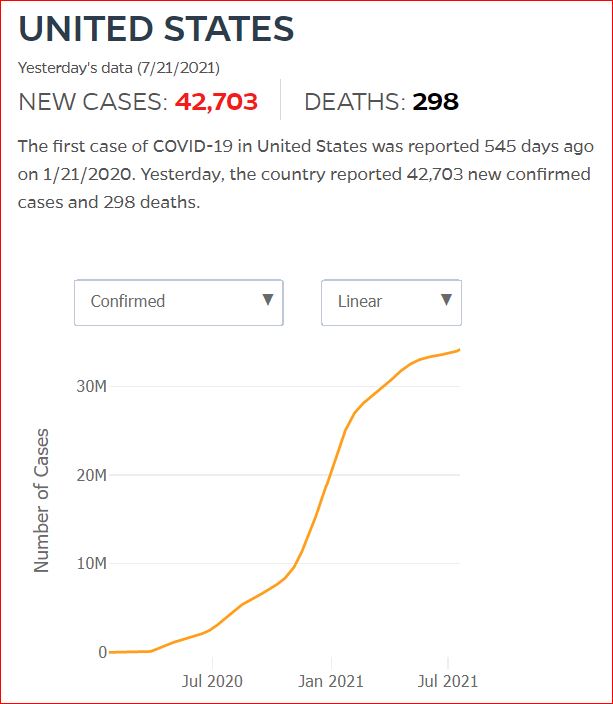
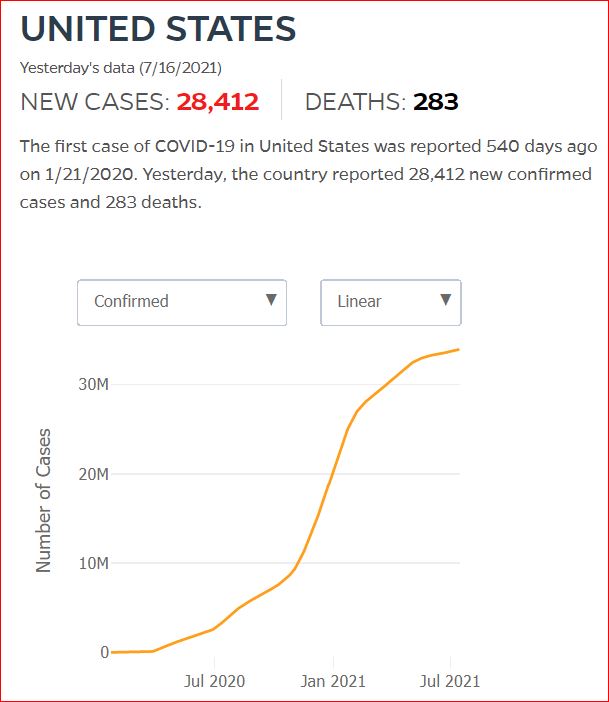
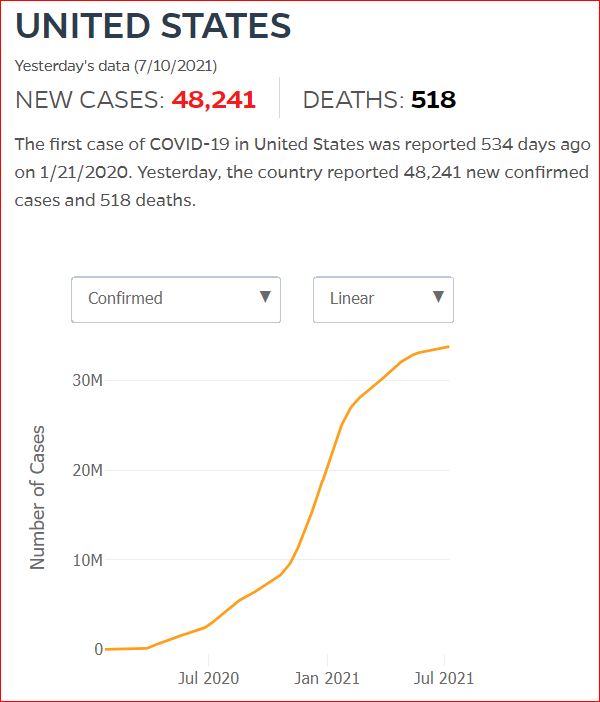
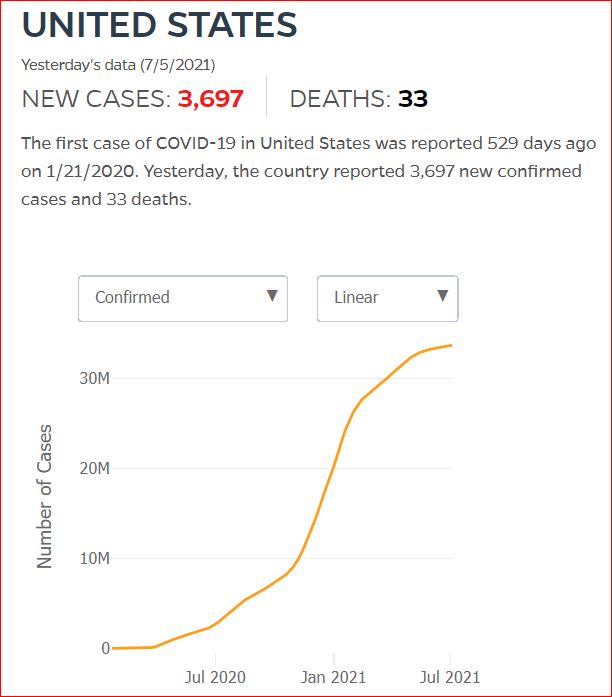
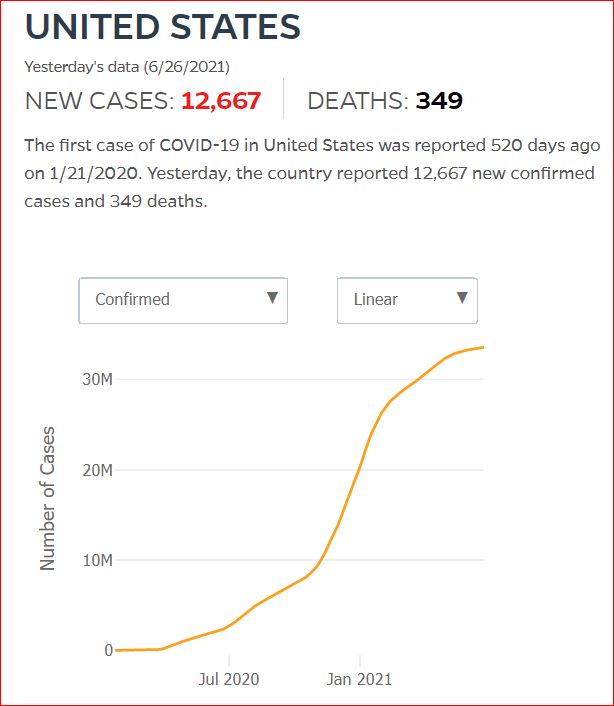
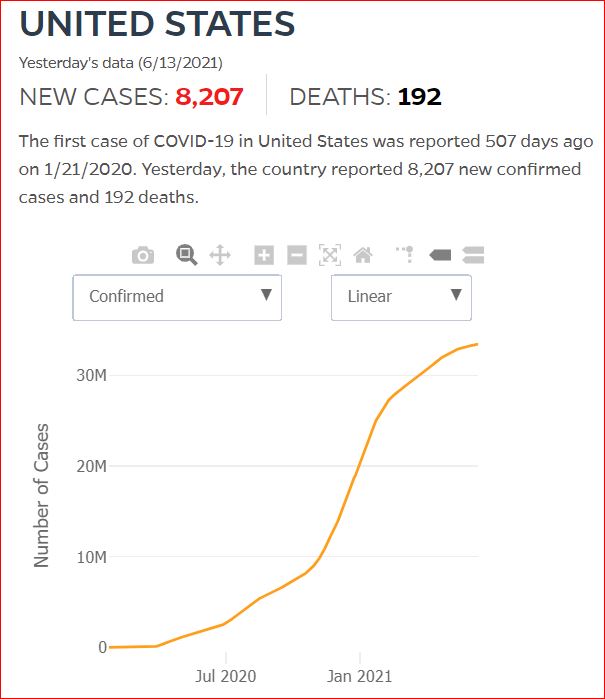
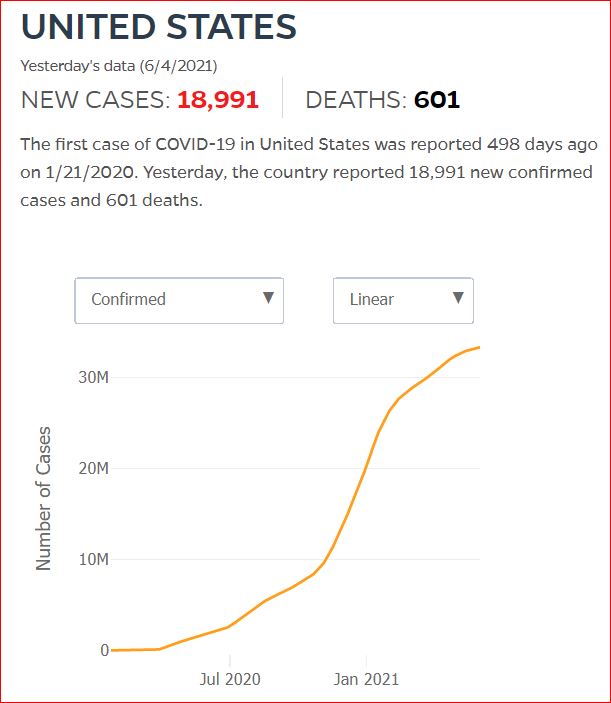
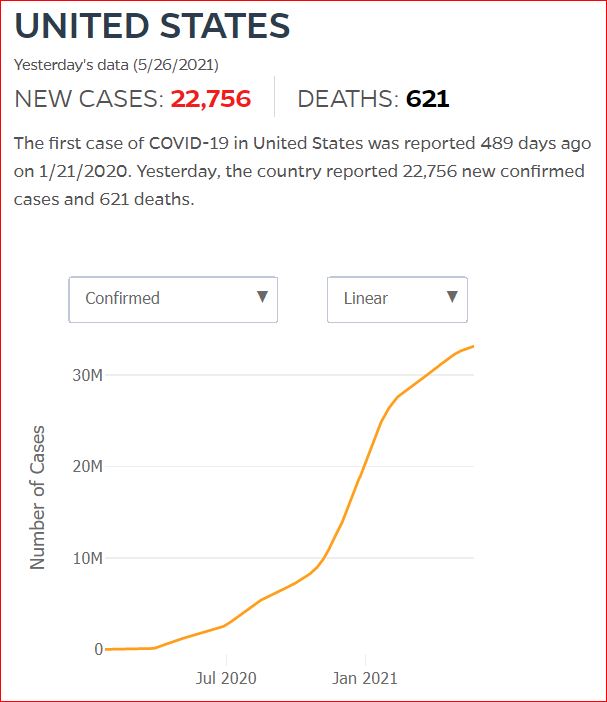
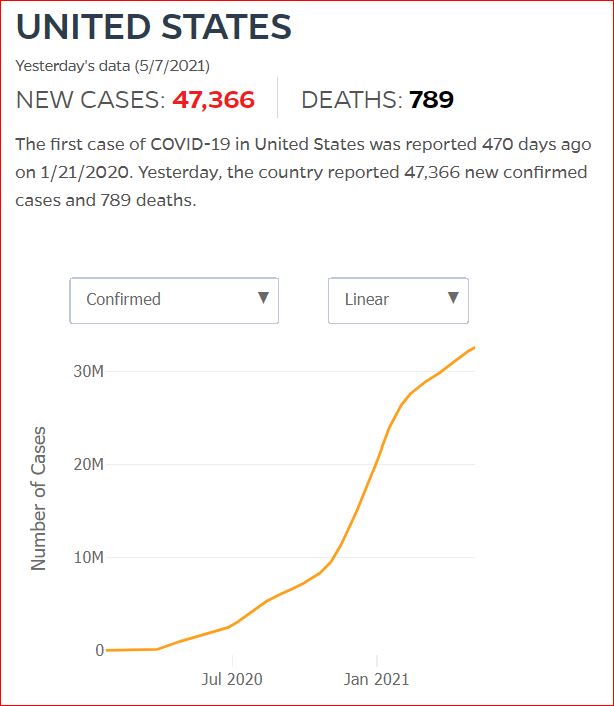
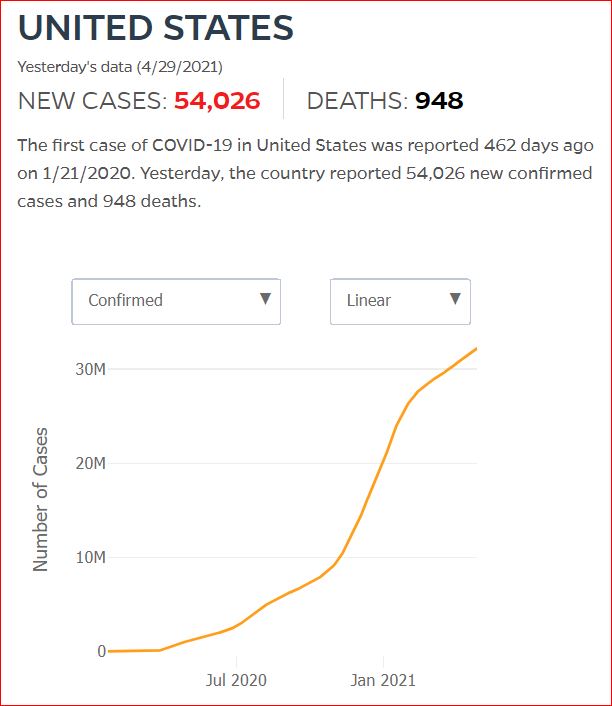
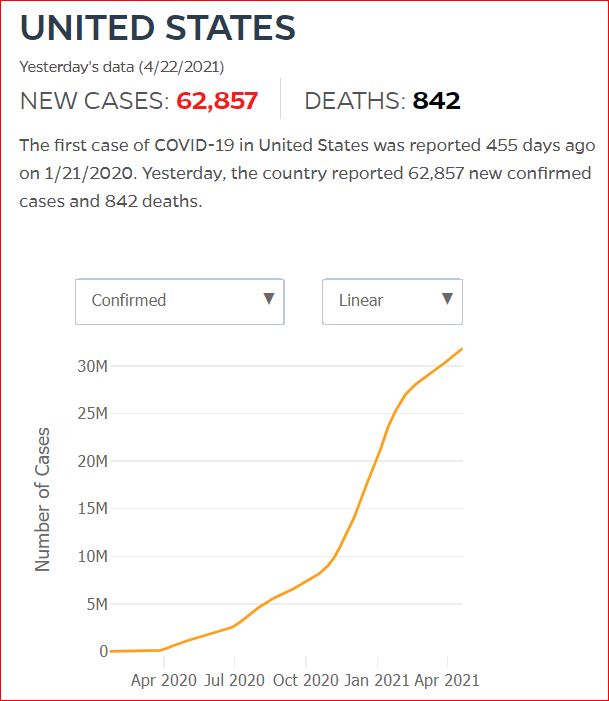
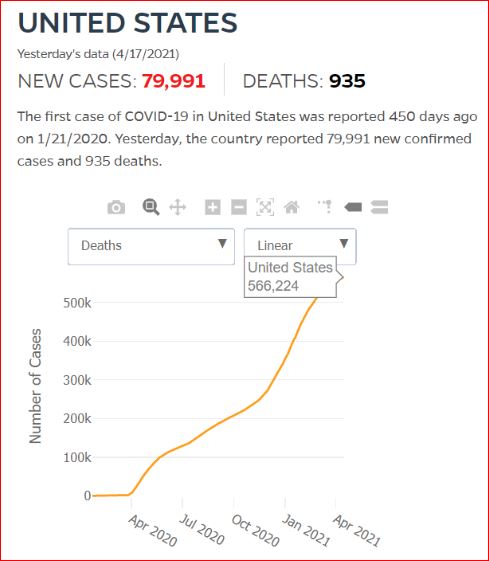
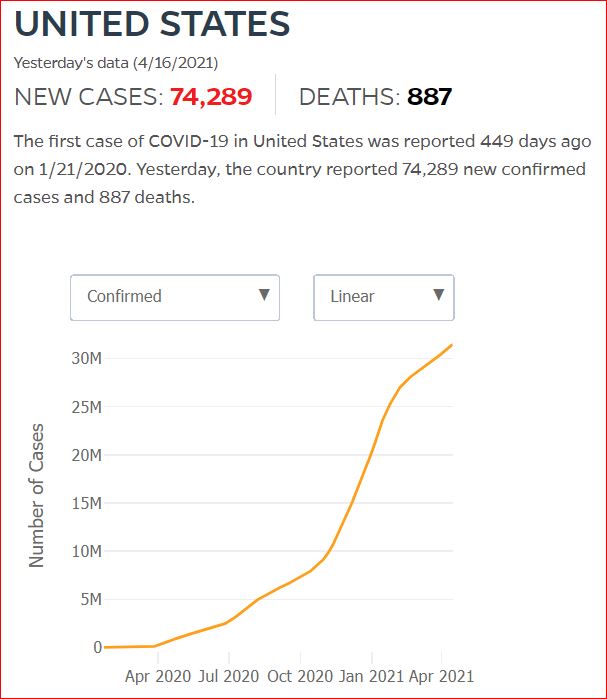
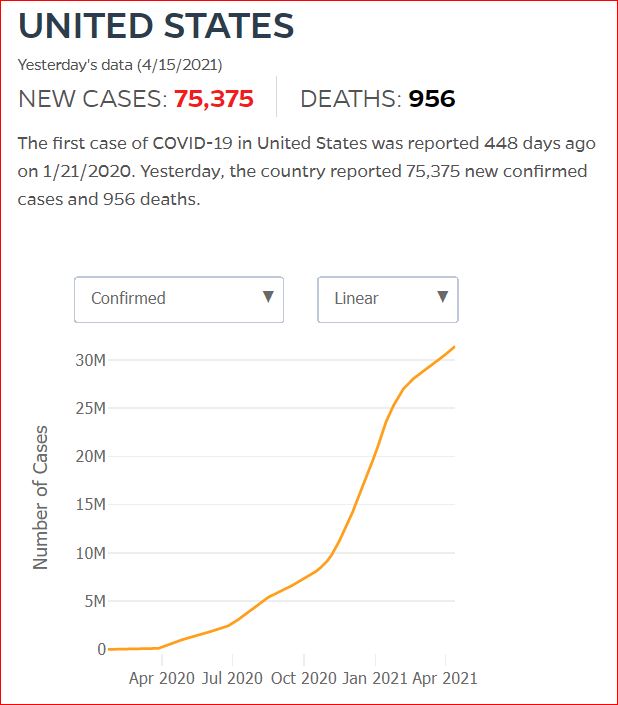
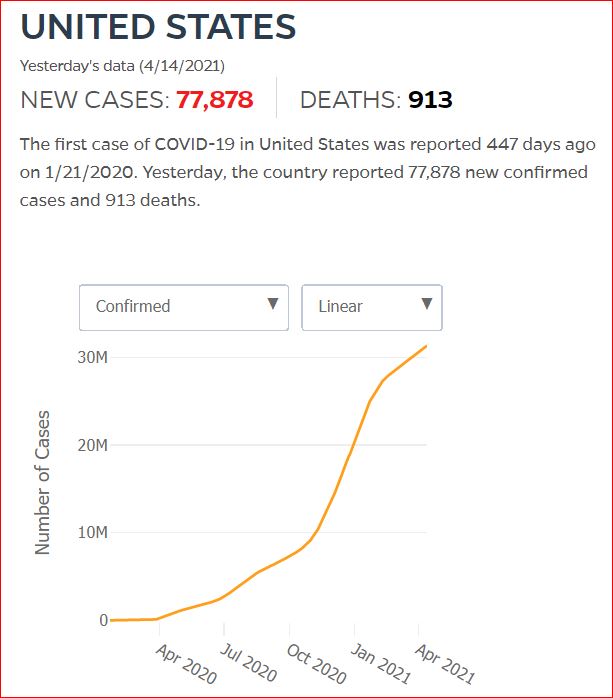
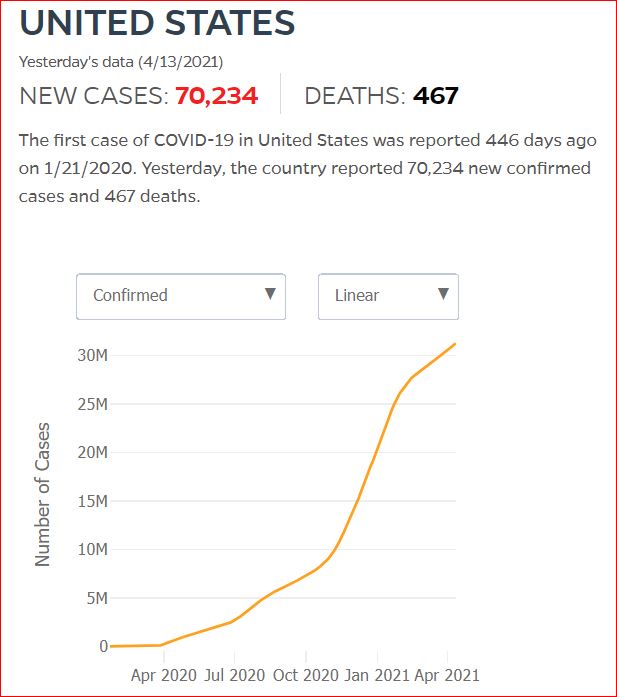
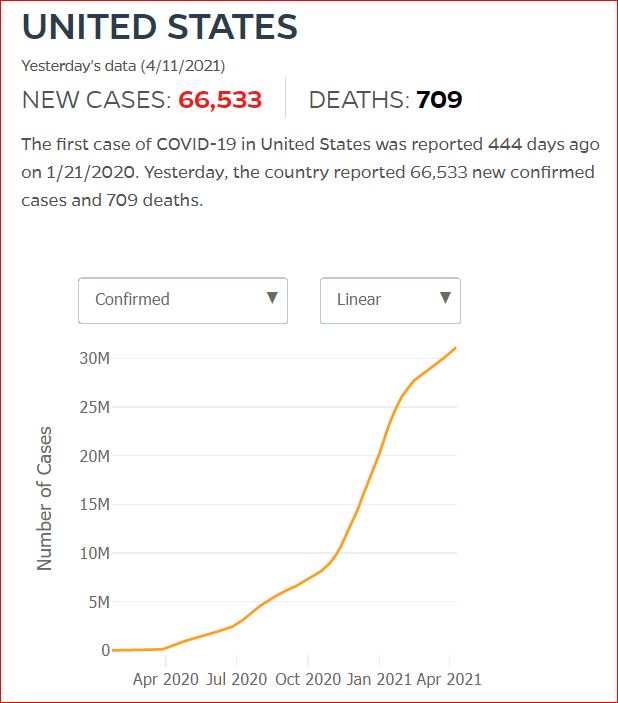
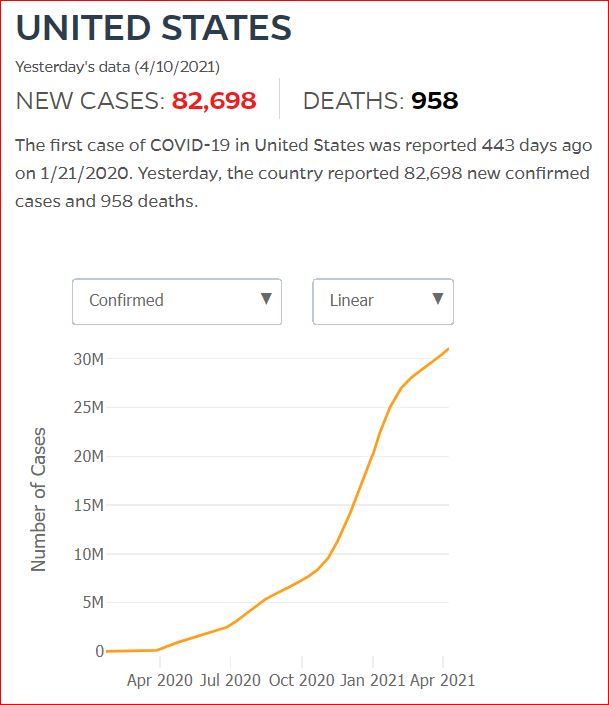
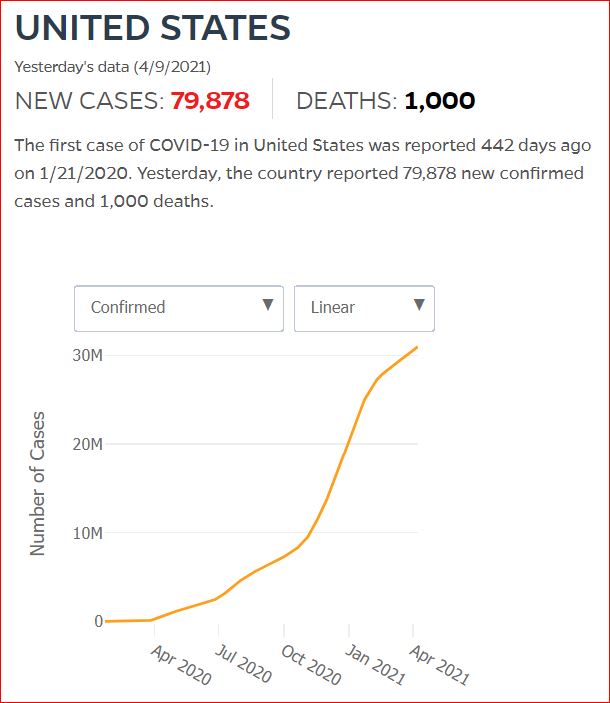
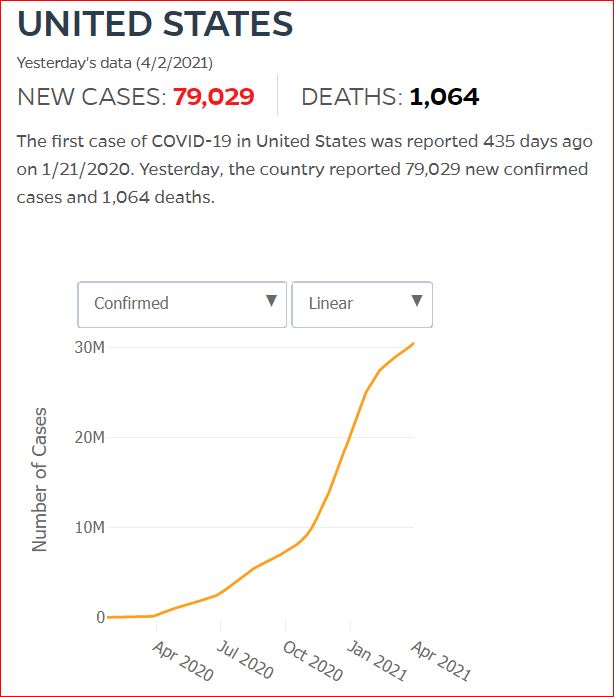
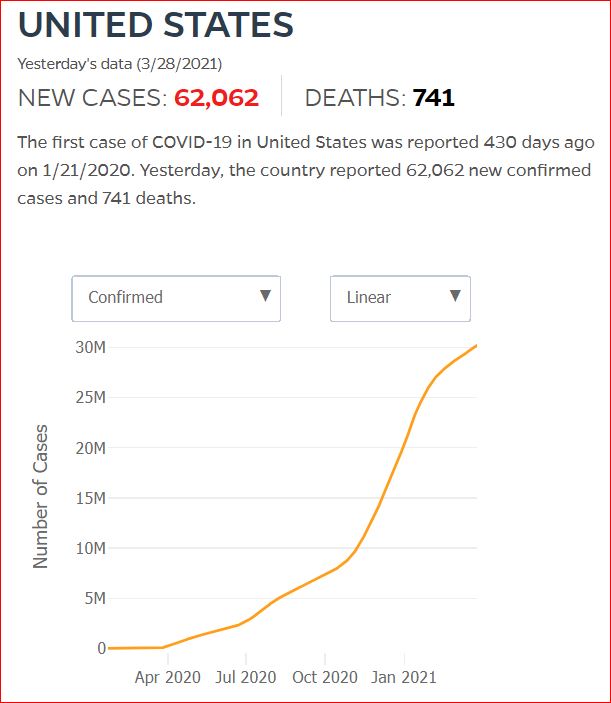
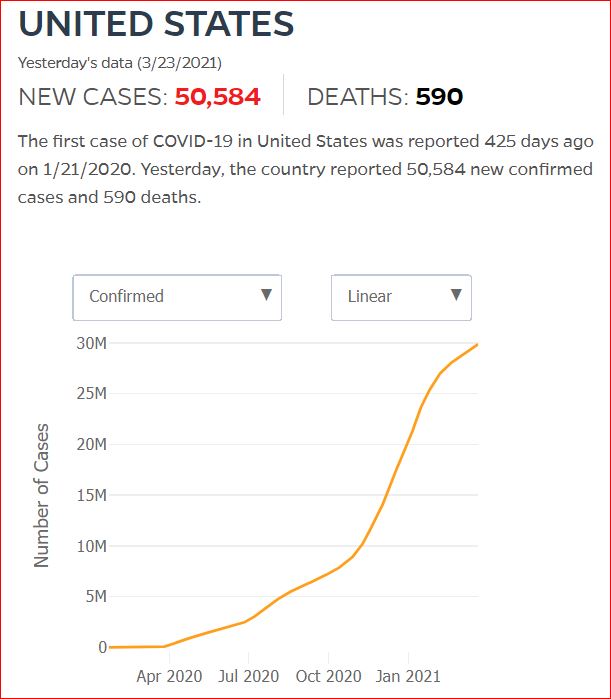
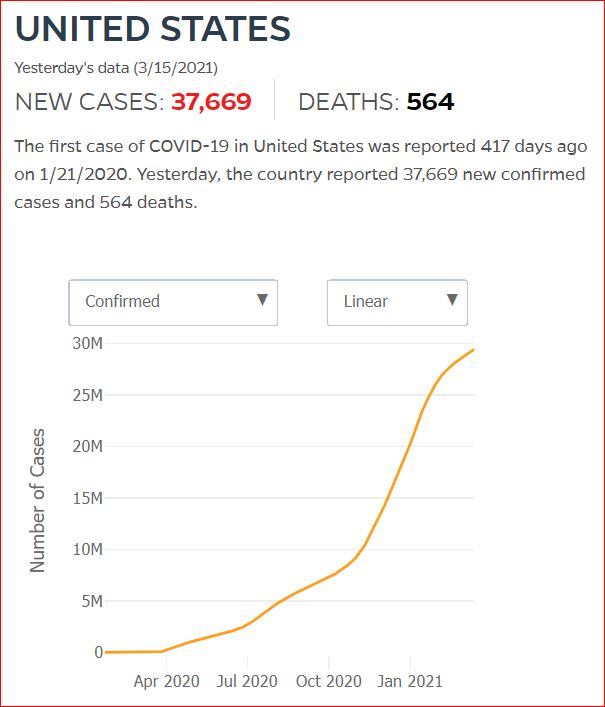
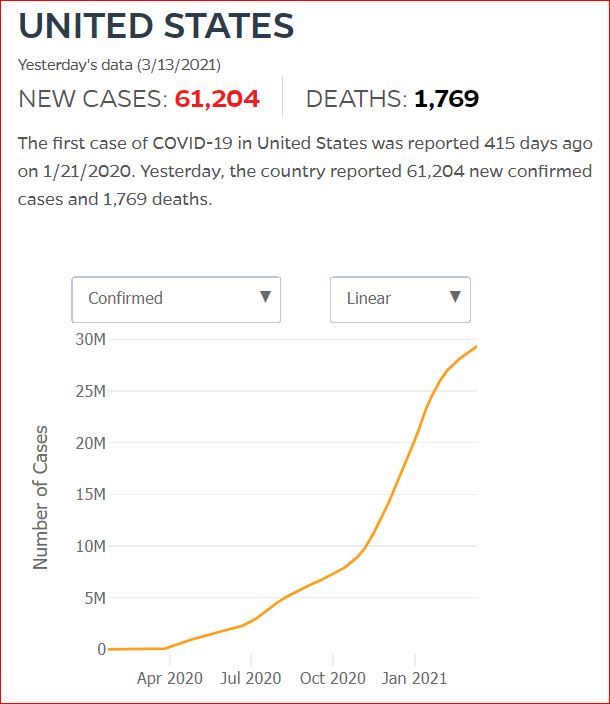
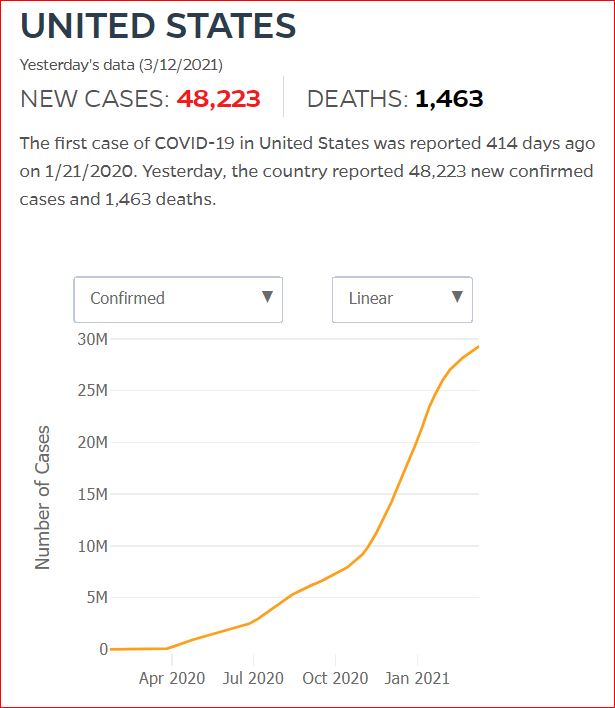
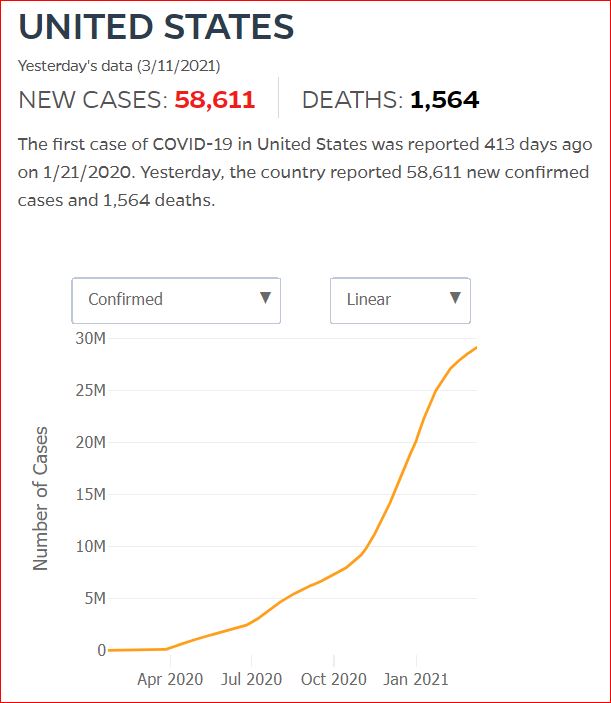
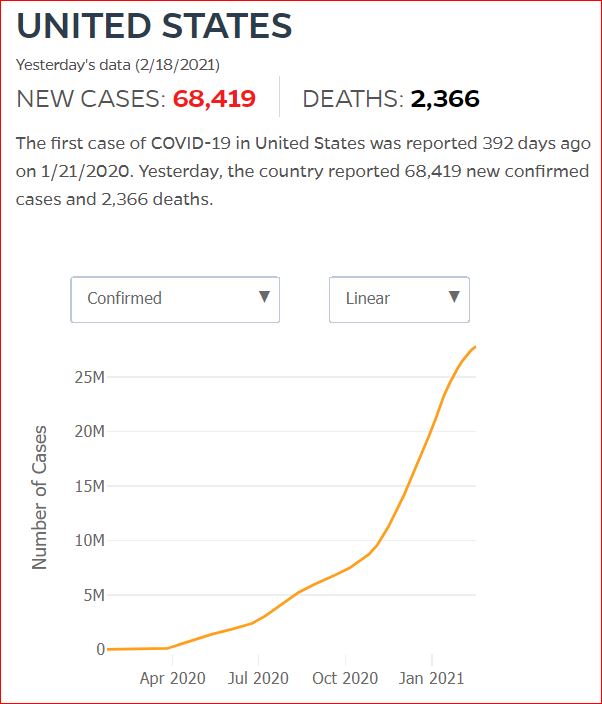
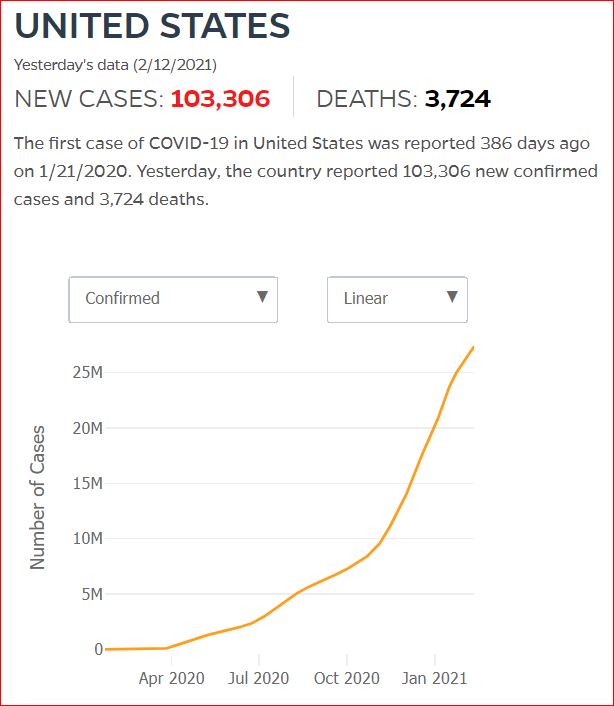
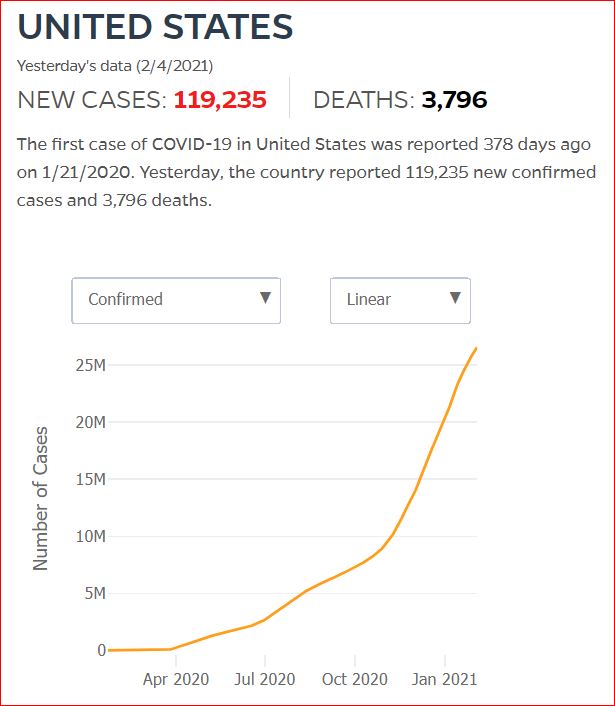
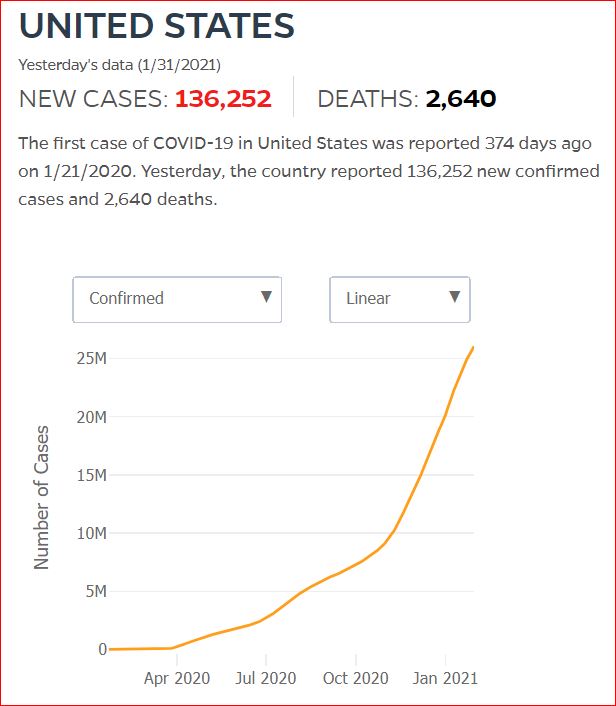
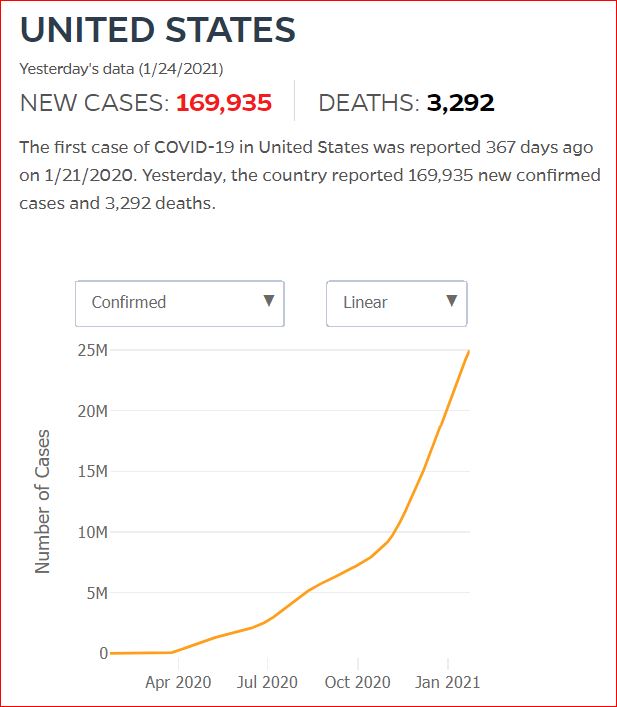
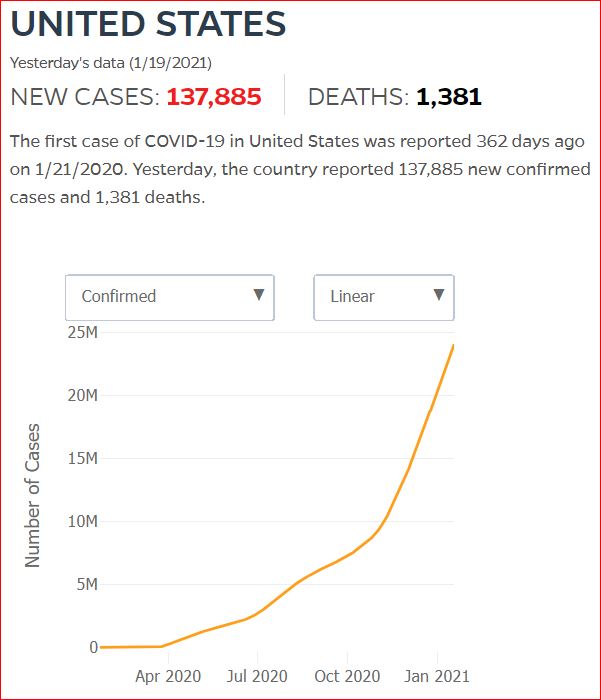
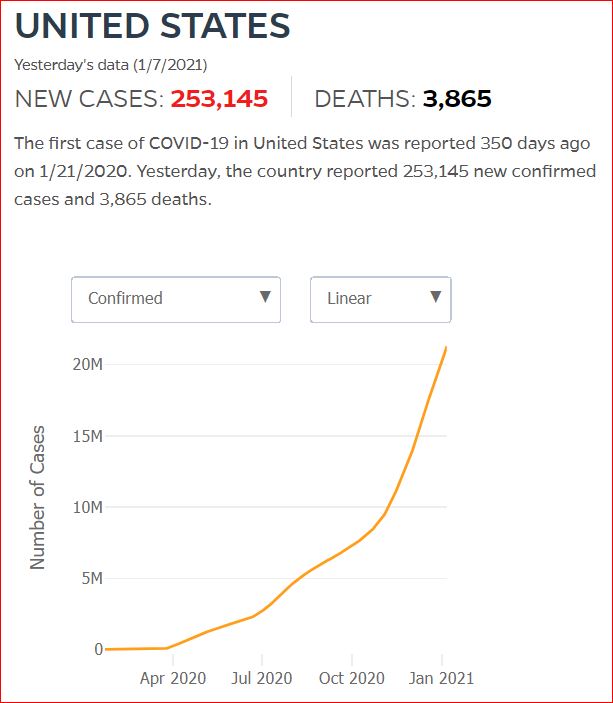
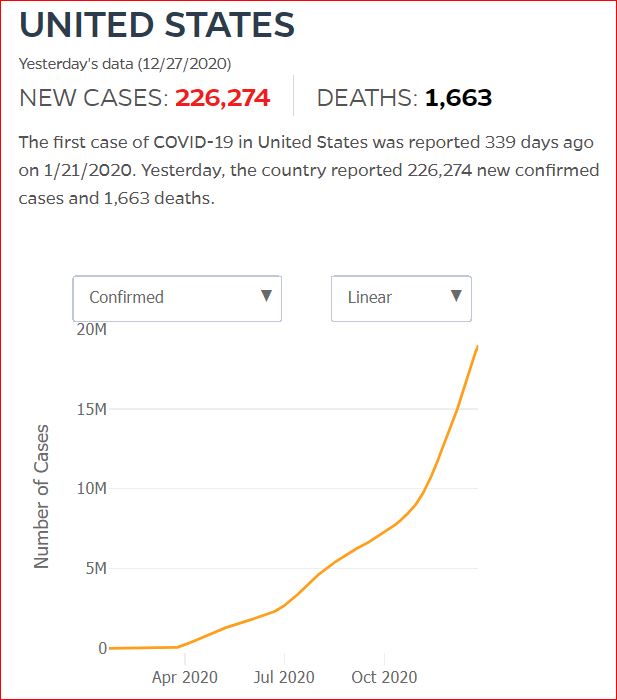
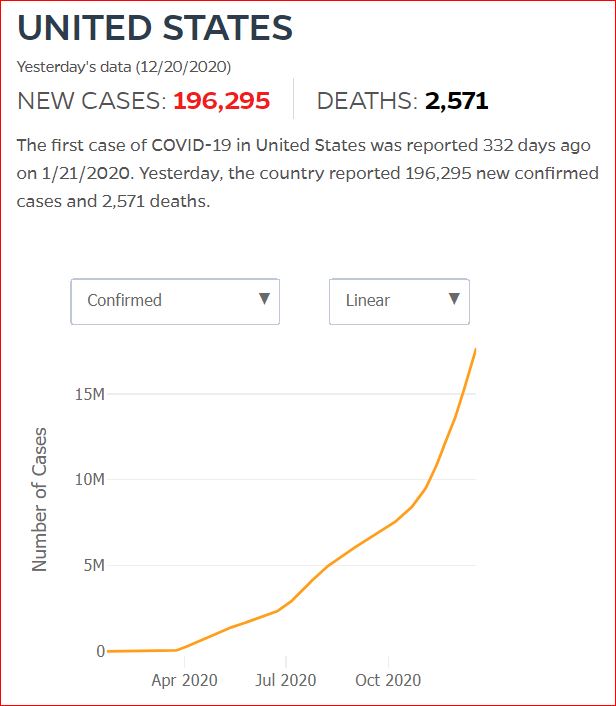
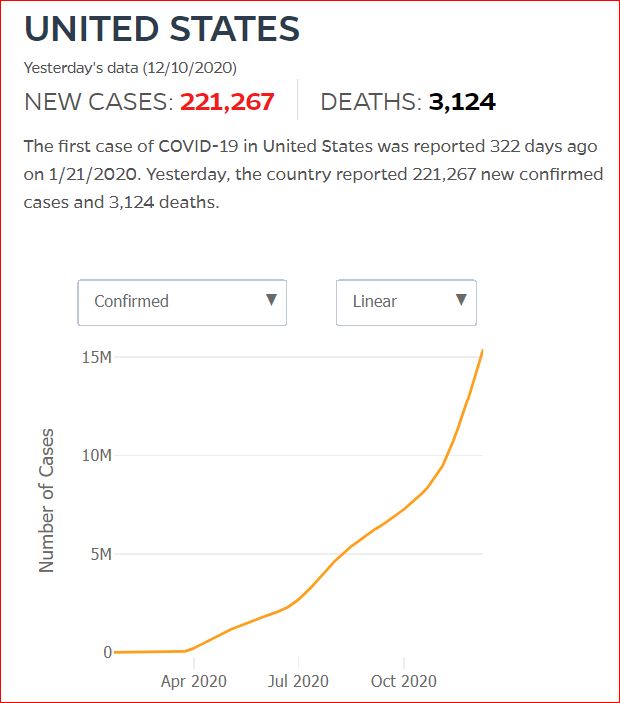
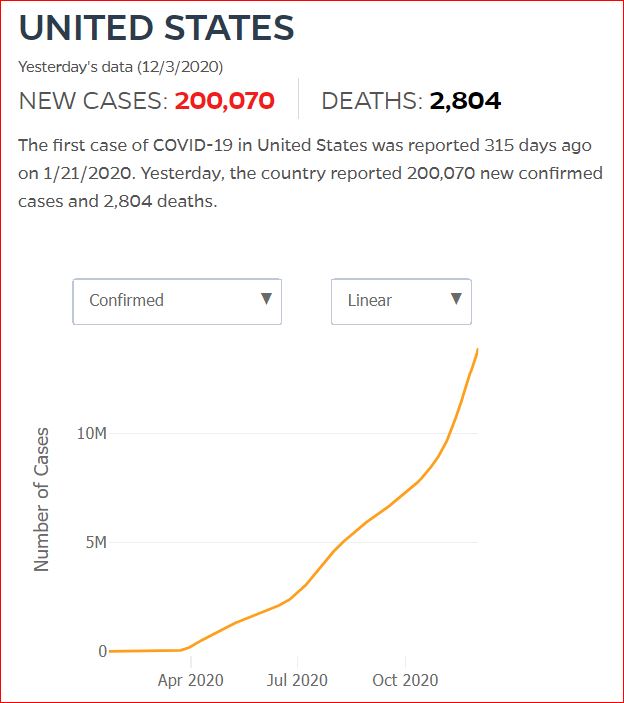
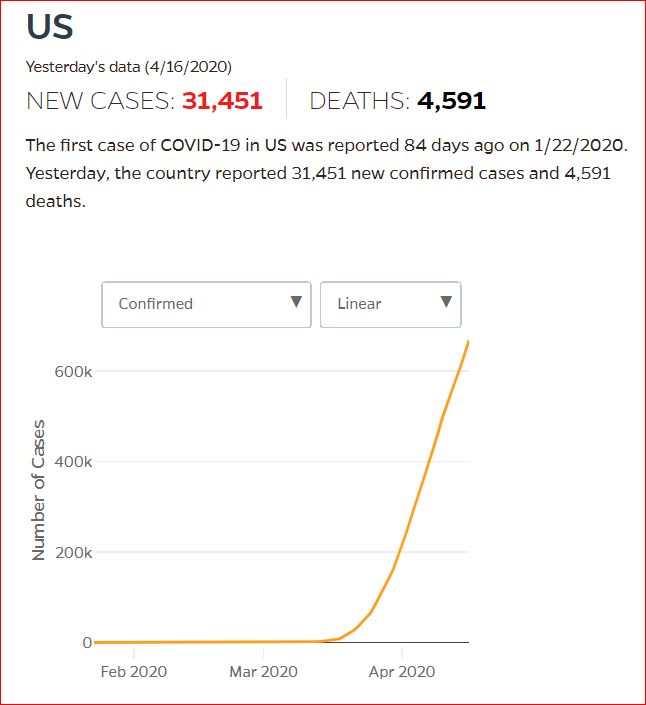
Yesterday's data (9/10/2021) New Cases: 145,081 Deaths: 1,926

The malevolent eyes? That's your 7th District Congressman, Tim Walberg.
He's earned infamy for sneering at vaccines and masks. @RepWalberg on Twitter.

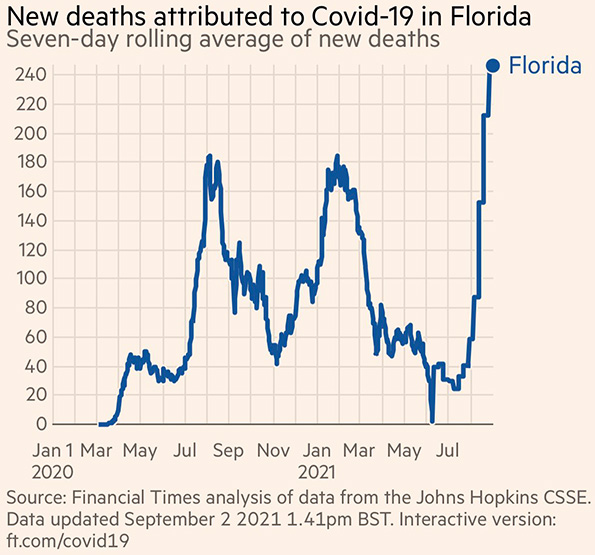
9/2/2021 Florida remains out of control. And remains the only state with daily COVID deaths higher than all previous waves. Over 2000 deaths in 10 days, by Vincent Rajkumar, Twitter, Financial Times
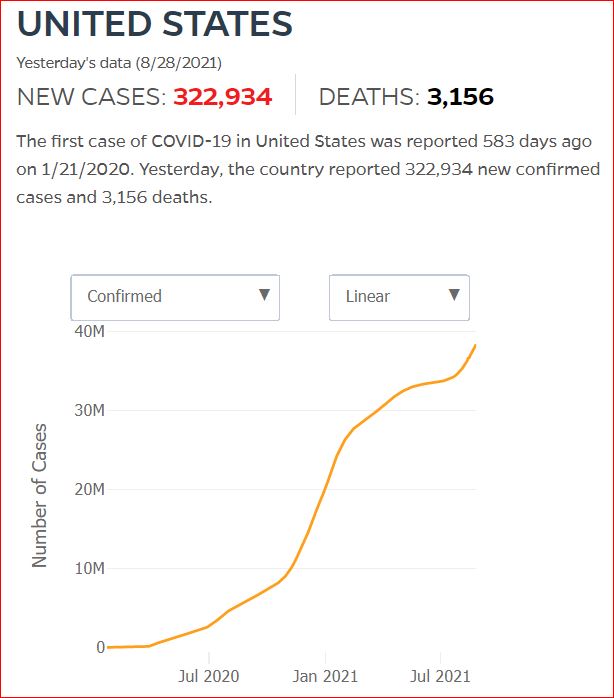
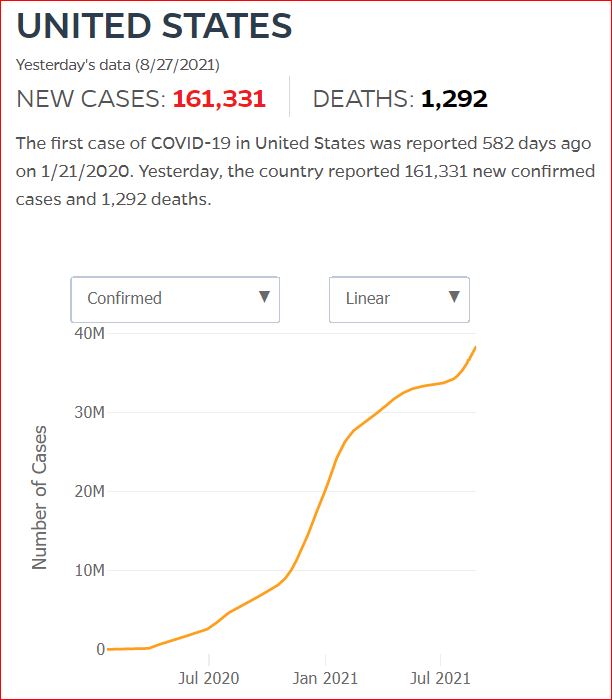
8/29/2021

8/29/2021

8/27/2021 Florida COVID update: 901 added deaths, largest single-day increase in pandemic history, by DEVOUN CETOUTE, Miami Herald
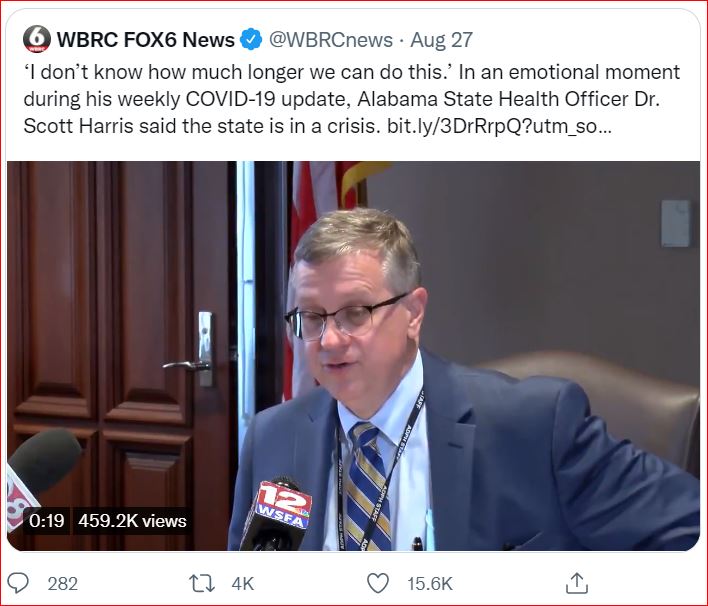
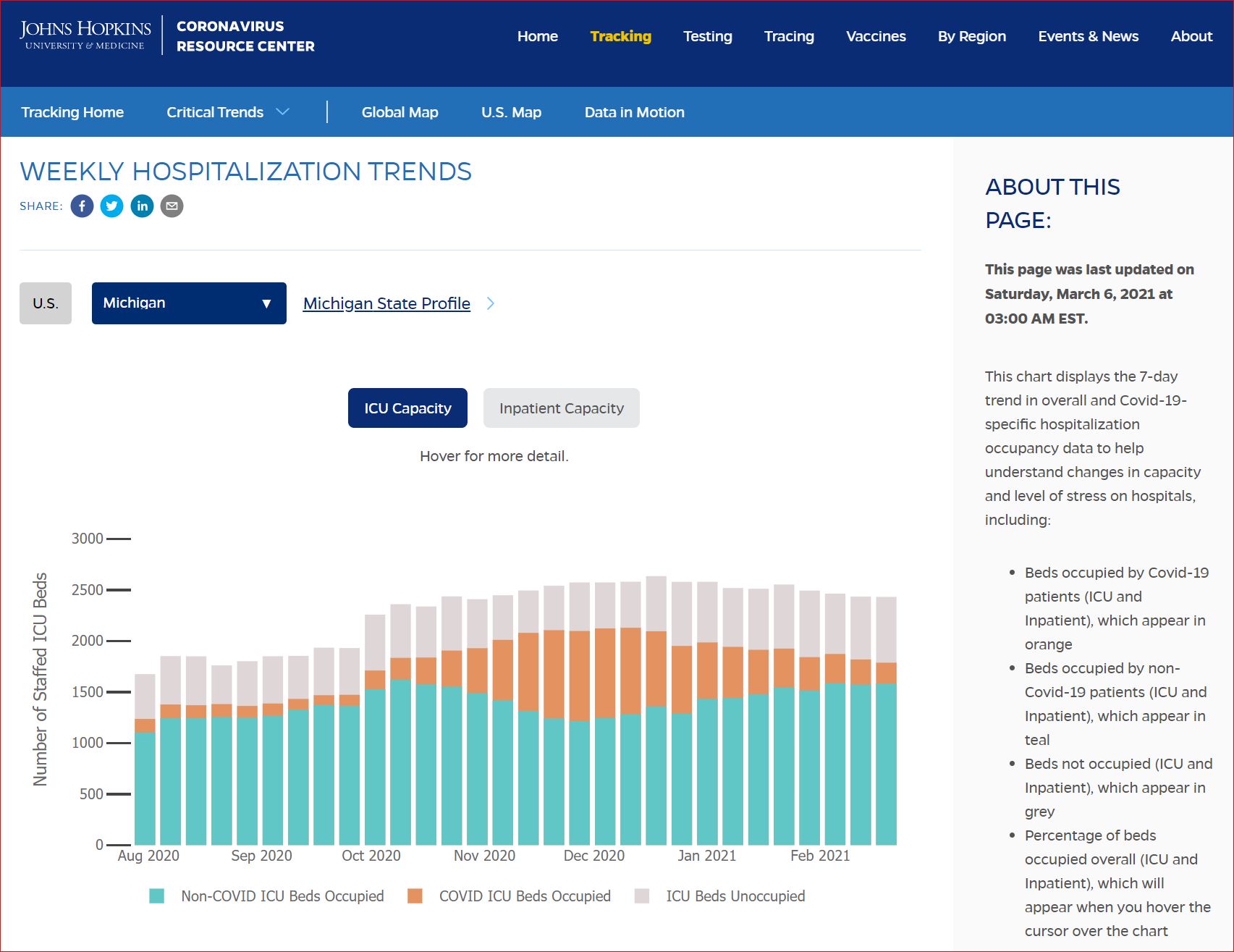
"We have negative ICU beds & that’s never happened before.
Alabama has 40 more ICU patients than we have ICU beds...
people are receiving ICU care in a hallway or in an ER."

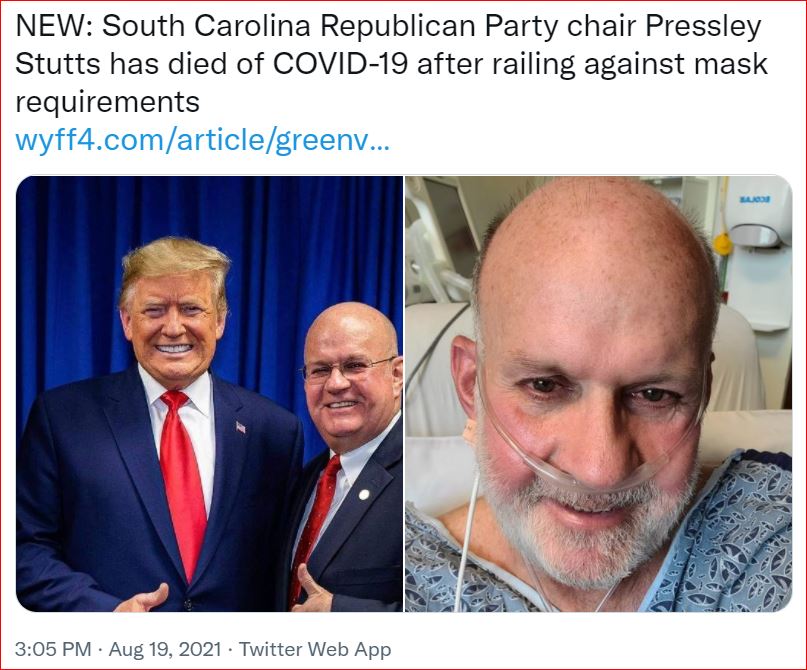
- WYFF NEWS, Greenville, South Carolina
Stutt's Facebook, August 13, 2021:
"Listen to me please: I am making a decision to go on a ventilator. This is my OWN decision.
I trust God to keep me. I ask you to trust Him, too. He IS ABLE, right?
My faith is strong that I will come through this. May be days or weeks,
but God IS in CONTROL!
Patty, I LOVE YOU! Pressley 3, Bart, Cavin and Linc, I LOVE YOU DEEPLY!
Remember what I have instilled in your hearts and minds.
I WILL wake up from this short rest and be back in the game soon!
PLEASE PRAY LIKE YOU HAVE NEVER PRAYERED BEFORE!
I HUMBLY ASK YOU. GOD BLESS ALL OF YOU!"
It wasn't a game.


8/15/2021: Florida hospital officials are seeing an influx of young, healthy adults filling their wards across the state, many requiring oxygen. In the past week in Florida, 36% of the deaths occurred in the under-65 population, compared with 17% in the same week last year when the state was experiencing a similar COVID surge. Florida is the national leader in coronavirus deaths, averaging more than 150 a day in the past week.

8/14/2021: "She was loved by all of her teachers. She was an honor student, a band student. Everybody says if they had 30 kids in the classroom like her, they have the perfect classroom," said Smith County Schools Superintendent Nick Hillman.
The eighth-grader died early Saturday morning, hours after Mississippi Gov. Tate Reeves downplayed the impact the virus has on kids.

8/10/2021: 'He went downhill so fast': 12-year-old boy in Texas dies after testing positive for COVID-19


Boundary Issue Impaired Trump Voters Die to Prove Loyalty




7/27/2021 Tennessee evangelical pastor demands churchgoers ditch their masks: ‘Don’t believe this delta variant nonsense’, by Jaclyn Peiser, The Washington Post
If “you start showing up [with] all these masks and all this nonsense, I will ask you to leave,” Locke, 45, told scores of Global Vision Bible Church parishioners during his sermon on Sunday. His statement was followed by cheers and applause.
“I am not playing these Democrat games up in this church,” he added.
Tennessee recently reported that 98 percent of people who died of covid and 97 percent of covid hospitalizations are among the unvaccinated.











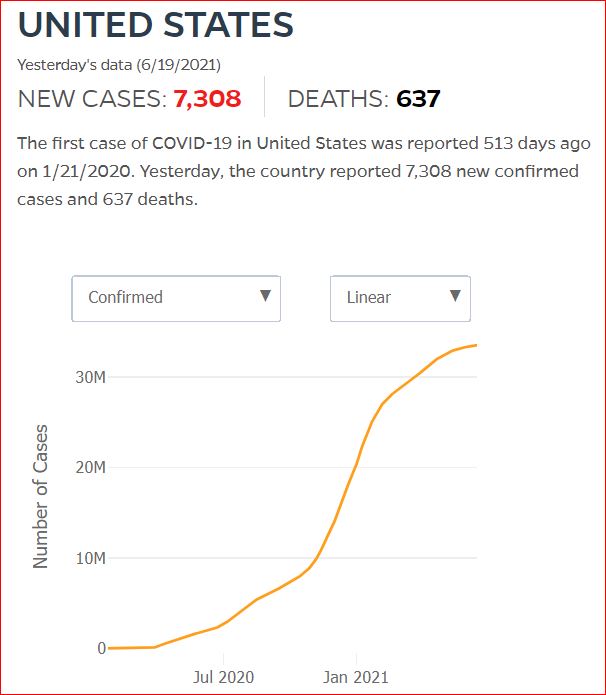


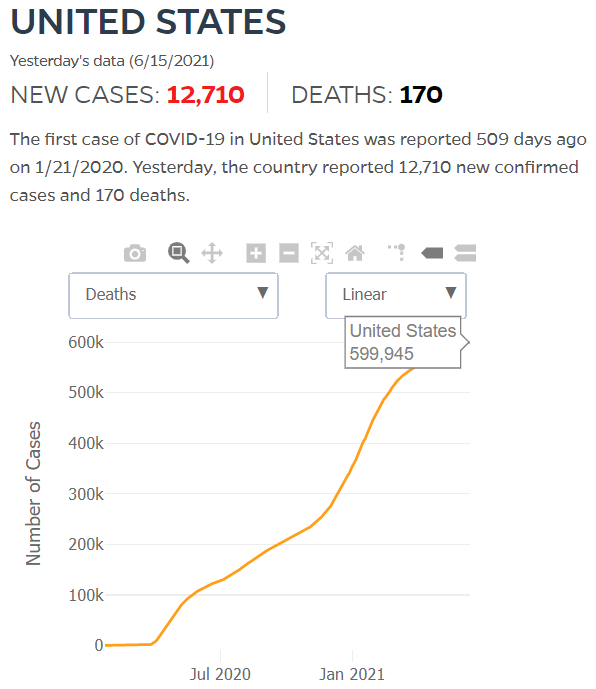
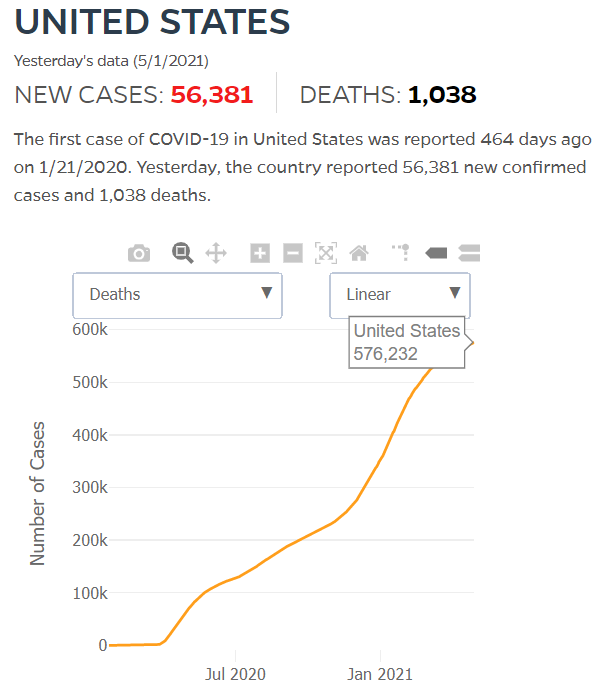
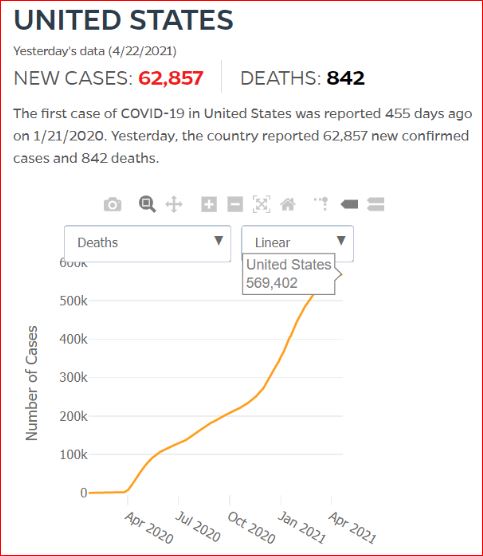
By JHU stats, yesterday America reached 599,945 Covid deaths. Other accountings say we long ago topped 600,000.


































560,000 Dead. Trump Voters Did This to America.
Live Rich, Die Old, Leave a Blood Trail of Nasty-Ass Quotes




3/28/2021 Birx, Who Gushed Over Trump’s Handling of Virus, Now Says He’s Responsible for Hundreds of Thousands Dead,
by Peter Wade, Rolling Stone
Birx: “There were about 100,000 deaths that came from that original surge.
All of the rest of them, in my mind, could have been mitigated or decreased substantially”

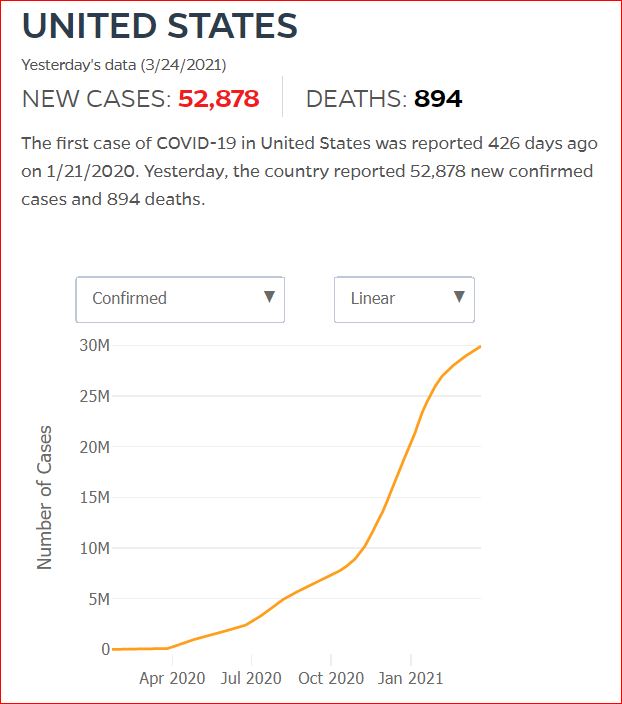




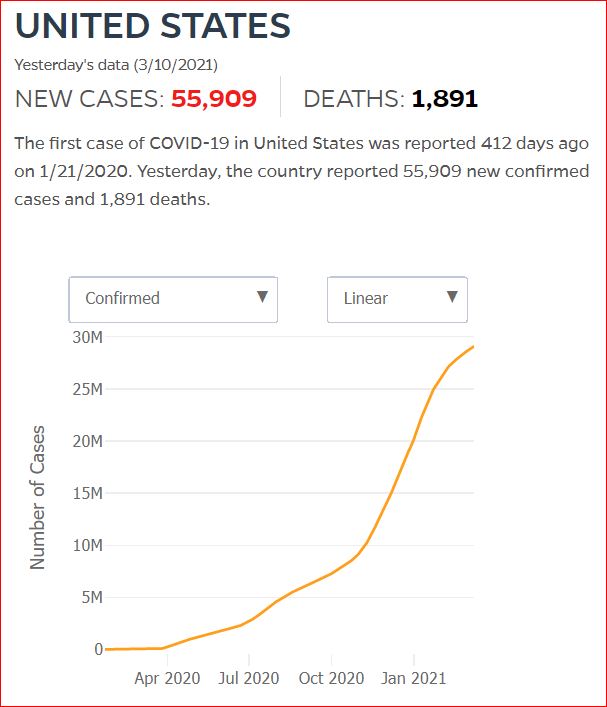
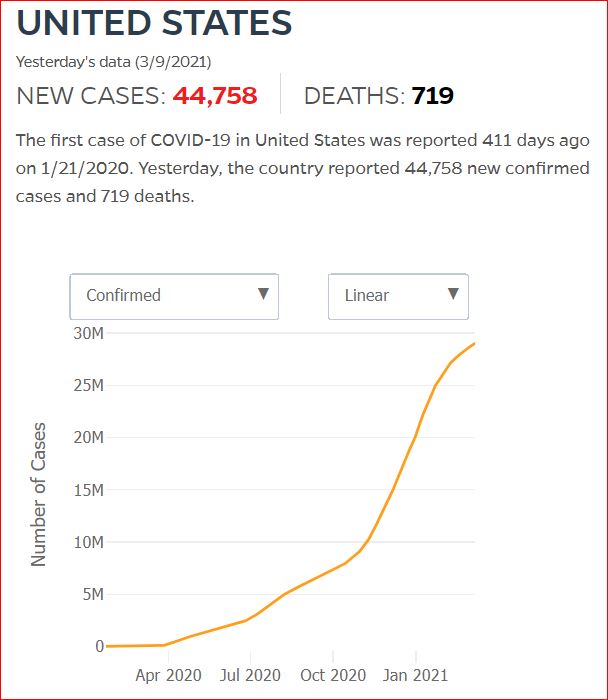

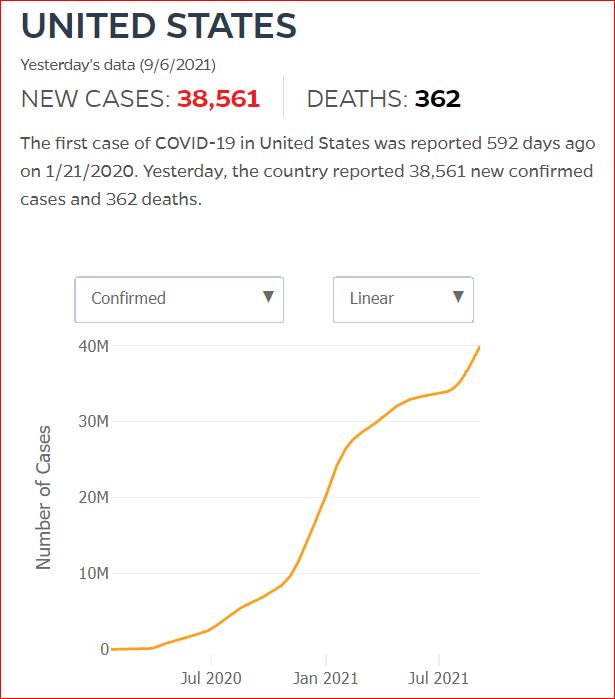
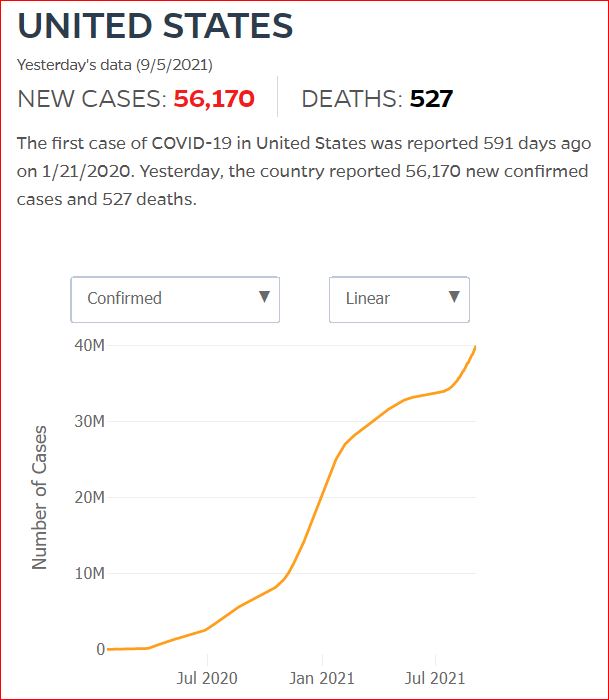
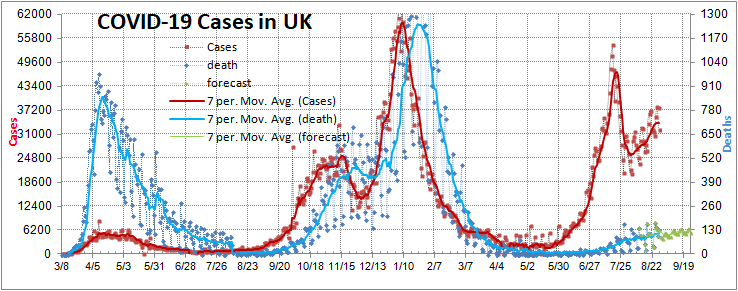
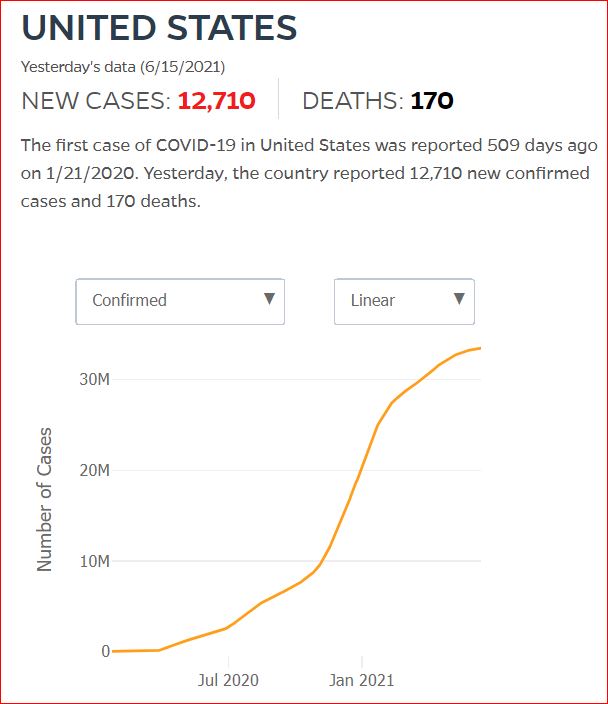
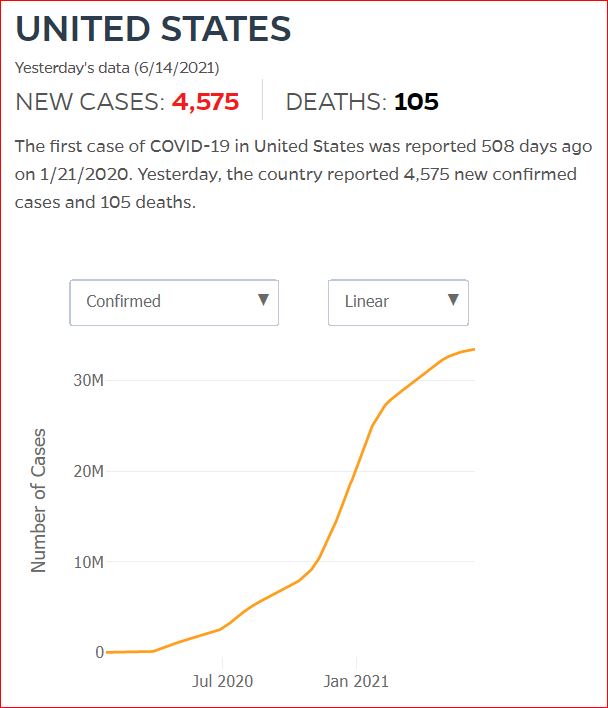
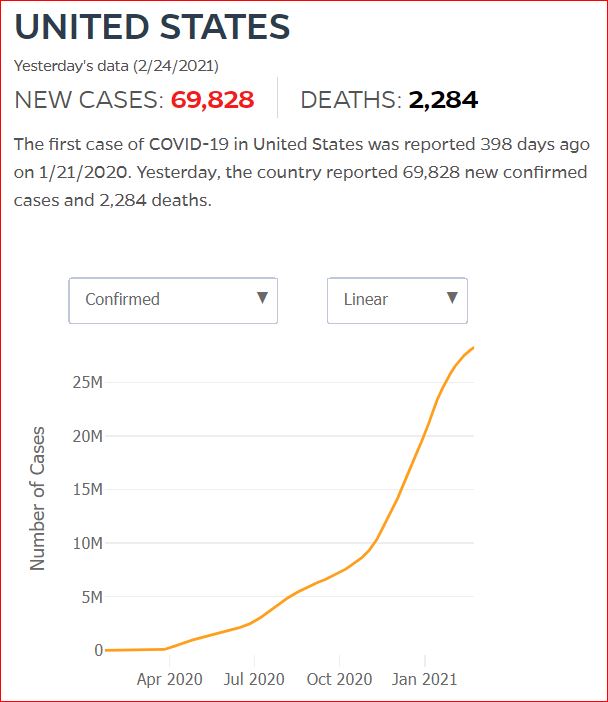
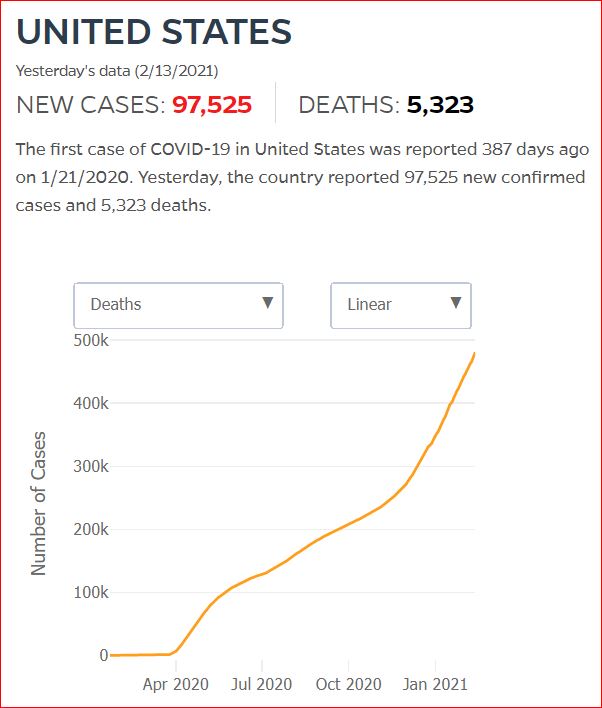
Click either of the above two Johns Hopkins charts to make them interactive
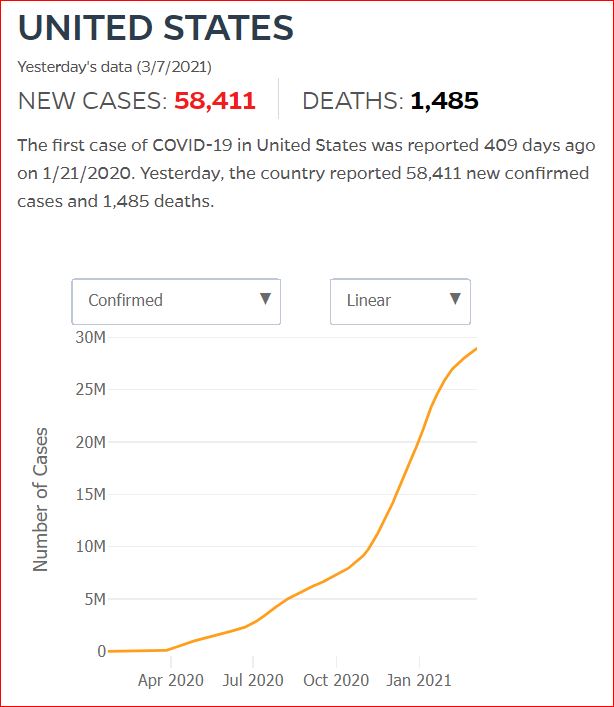

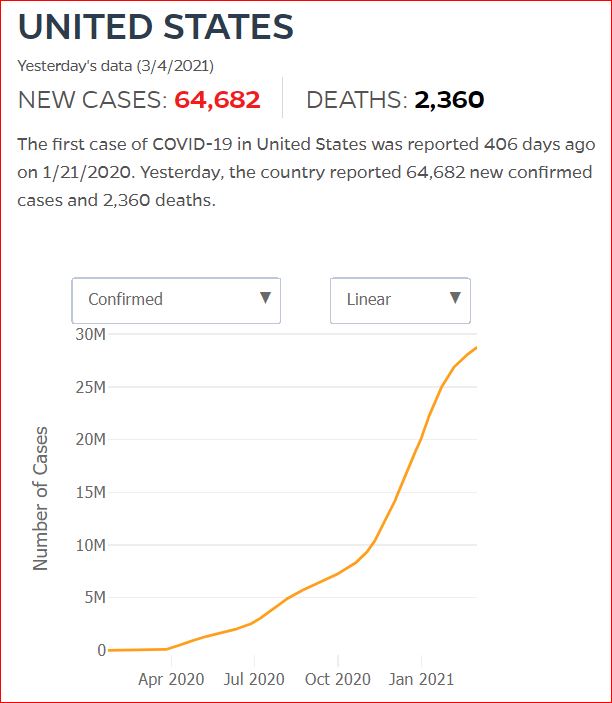
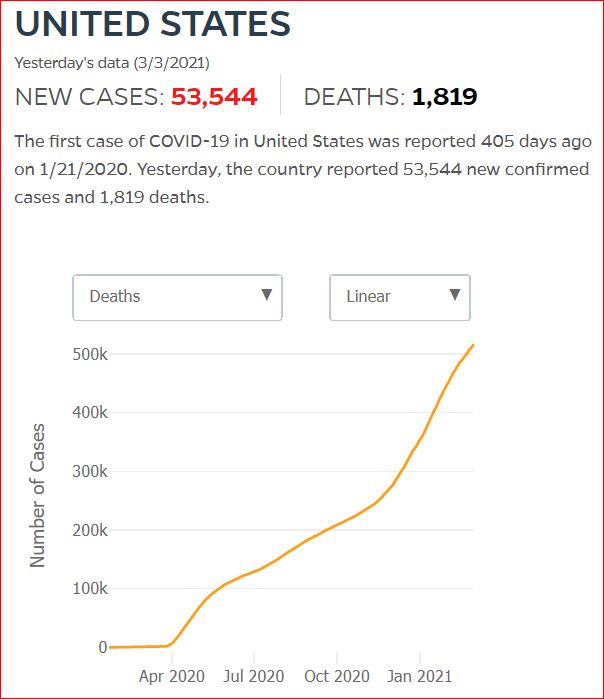


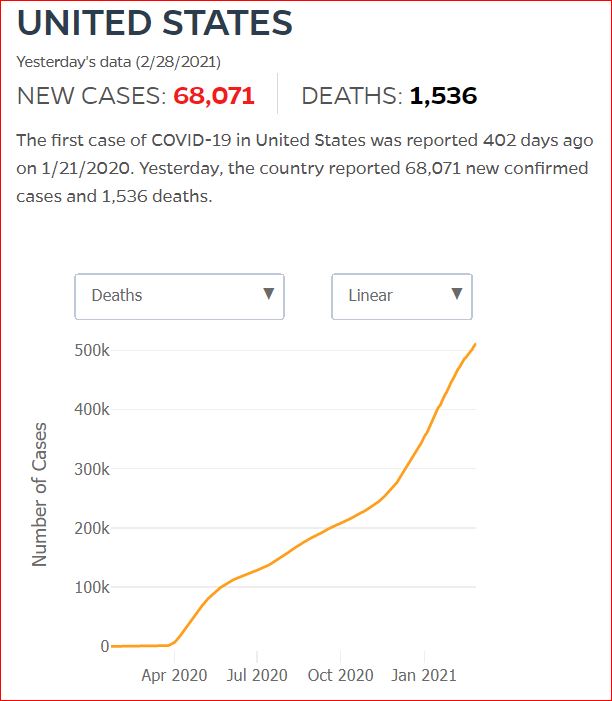
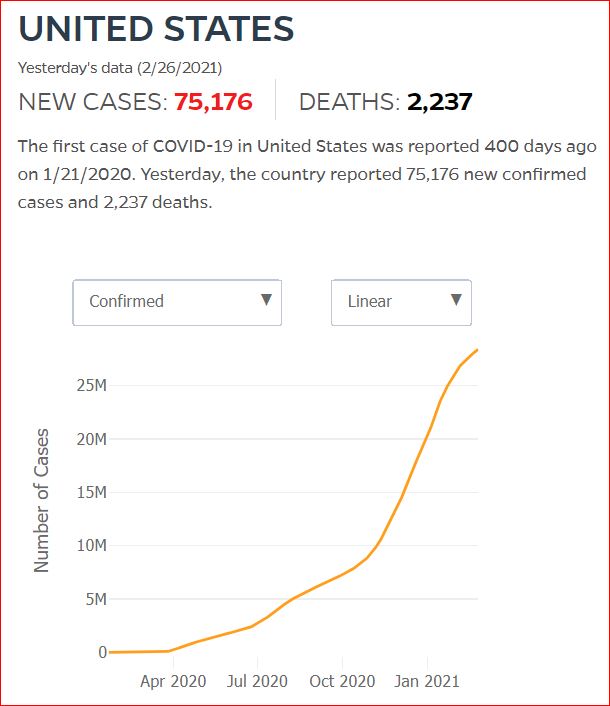
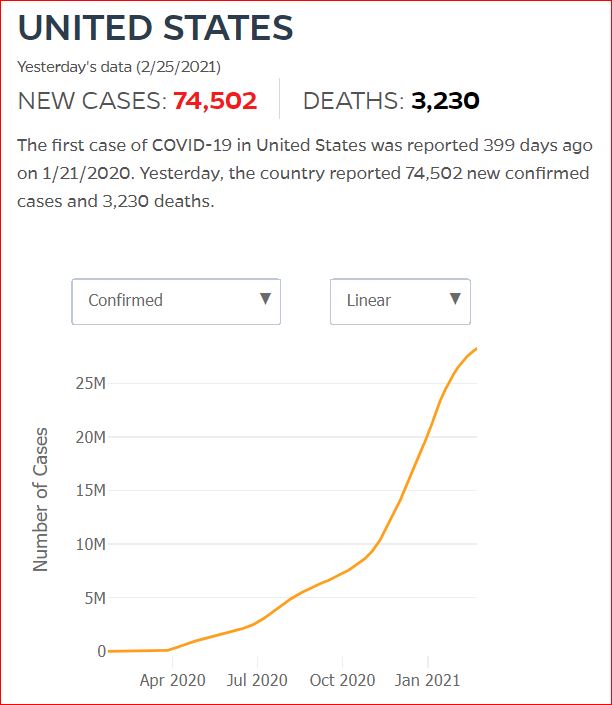
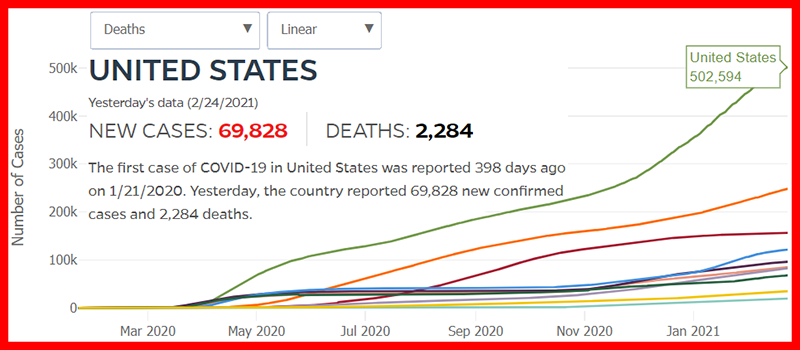
Yes, that's 502,594 officially dead of Covid-19







"- dressed in a little brief authority, most ignorant of what he's most assur'd"
2/11/2021 US could have averted 40% of Covid deaths, says panel examining Trump's policies, by Amanda Holpuch, The Guardian U.S.
The US could have averted 40% of the deaths from Covid-19, had the country’s death rates corresponded with the rates in other high-income G7 countries, according to a Lancet commission tasked with assessing Donald Trump’s health policy record.
Almost 470,000 Americans have died from the coronavirus so far, with the number widely expected to go above half a million in the next few weeks. At the same time some 27 million people in the US have been infected. Both figures are by far the highest in the world.



J. F. C.




Choose. Truth.
There. Was. No. Plan.






Wars, Pandemic or Insurrection, Republicans will find a way to kill you dead.


Death doesn't take Sundays off, but some of its statisticians do. Sad that 1800 deaths looks like an improvement.






The numbers speak for themselves. The numberless dead cannot.

Even those as senseless as Trump voters may finally be sensing a pattern

Another Proud Day in the Proud History of Proud Trump Voters
Another proud moment for Trump's proud voters. A record breaking cull.

Trump is playing golf. Pence is sking. 1 million of the promised 20 million vaccinations have happened.
Death Reporting Takes a Holiday

Hate if You Love Trump
 Through Trump's Hate, Darkness
Through Trump's Hate, Darkness
There ought to be words


Where are the words?
This is 47 times as many as were murdered in the 2017 Las Vegas bump stock shooting rampage.

A Good Trumper is a Trumper Who Stays Trumped.
But you're worrying about the imaginary rigged election, right?!!

"A Good Sucker is a Sucker Who Stays Stupid."



'Owning the libruls' with a Mass Casualty Event every day.
For what shall it profit a man, if he shall gain the whole world, but lose his own soul?
Mark 8:36 KJV

"Send not to know for whom these losers died. They died for Donald J. Trump."
 Were they as proud to die for Trump as Trump voters were willing to hate?
Were they as proud to die for Trump as Trump voters were willing to hate?
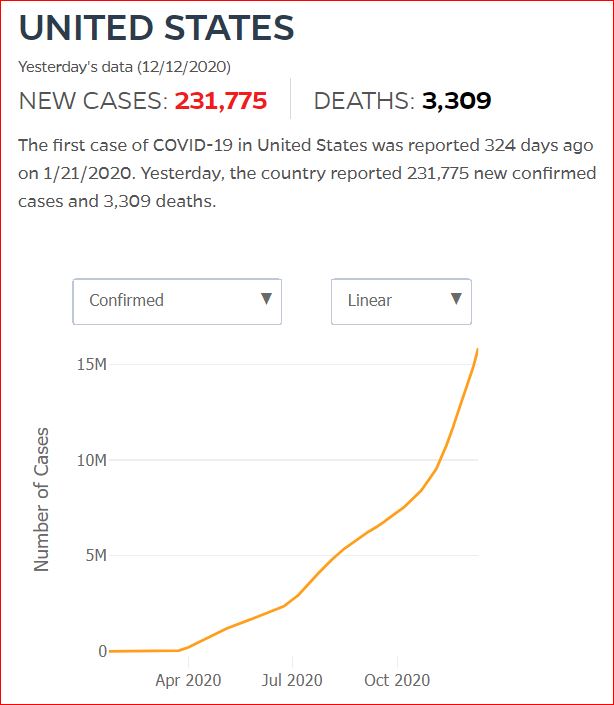
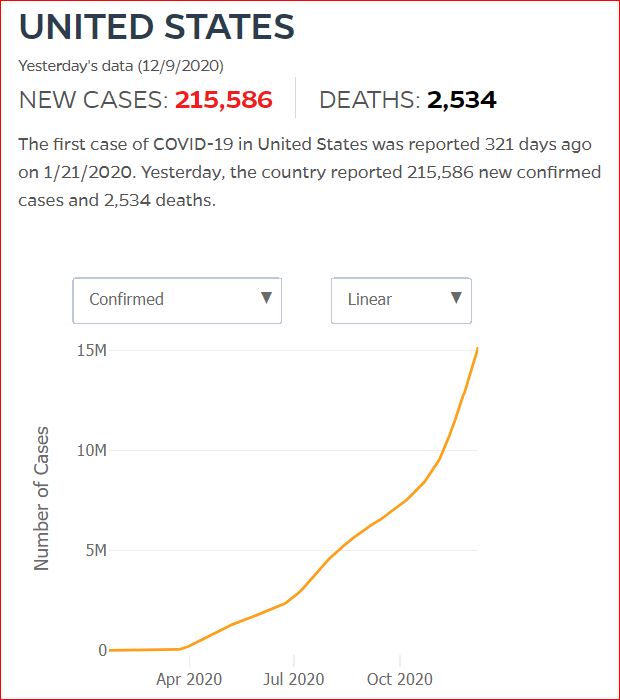 2,534 died December 8th
2,534 died December 8th
My Aunt Millie's boyfriend was one of these deaths.
In 22 days, ~1.8% of this day's 215,586 new cases -
3,881 more men and women, boys and girls, grandmothers and grandfathers, mothers and fathers, brothers and sisters, aunts and uncles, cousins and nieces and nephews - will have died.



A CoronaViral Advent Calendar
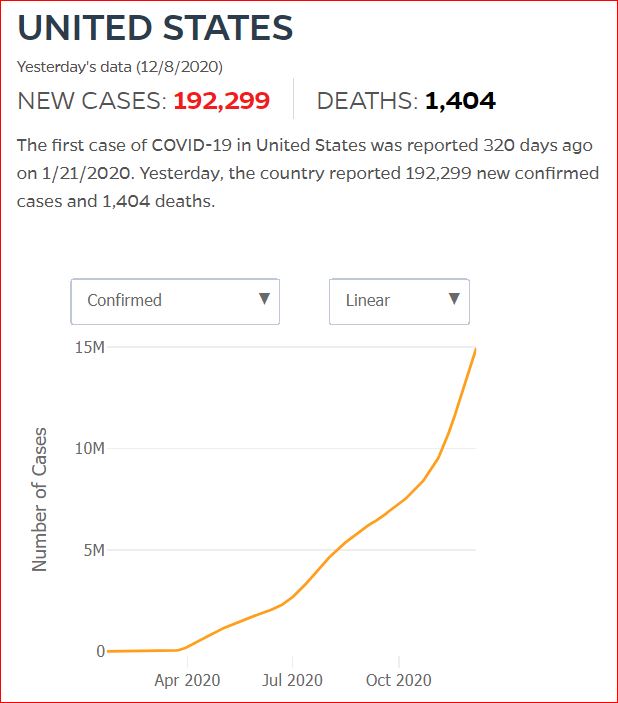
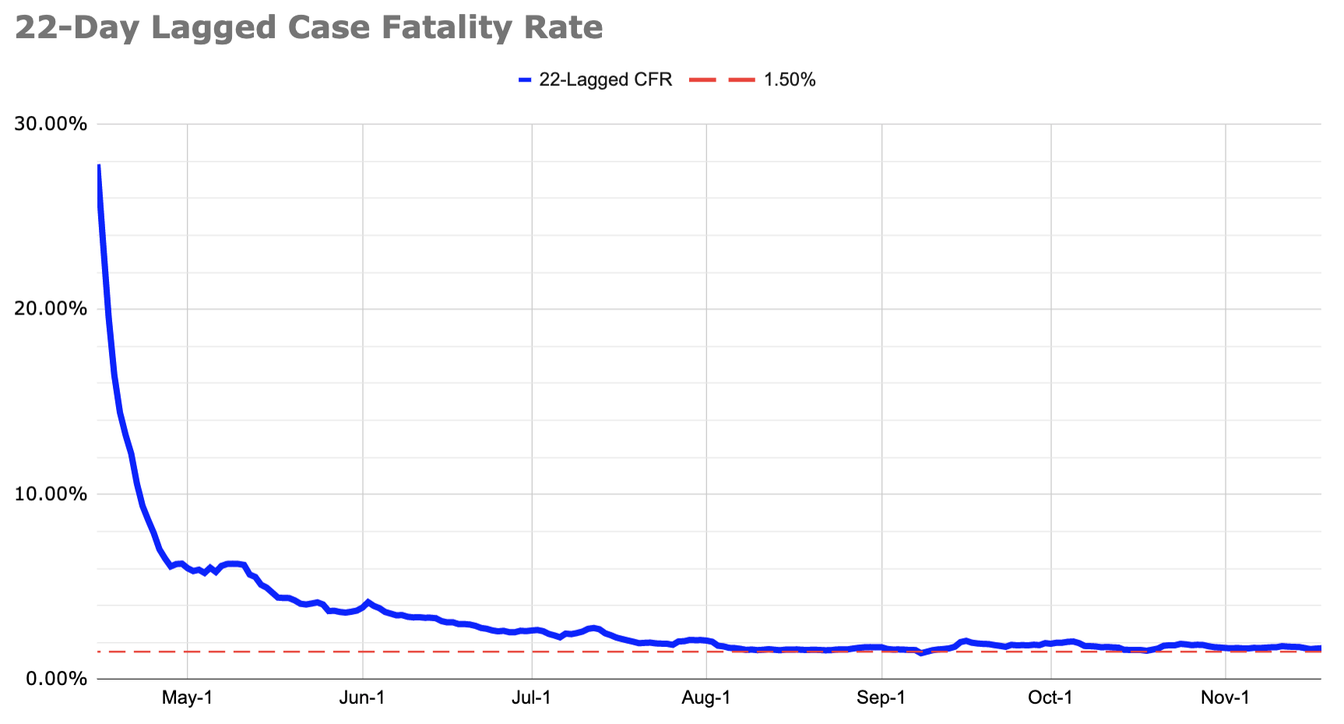 At last estimate, the 22 day lagged case fatality rate was 1.8%
At last estimate, the 22 day lagged case fatality rate was 1.8%
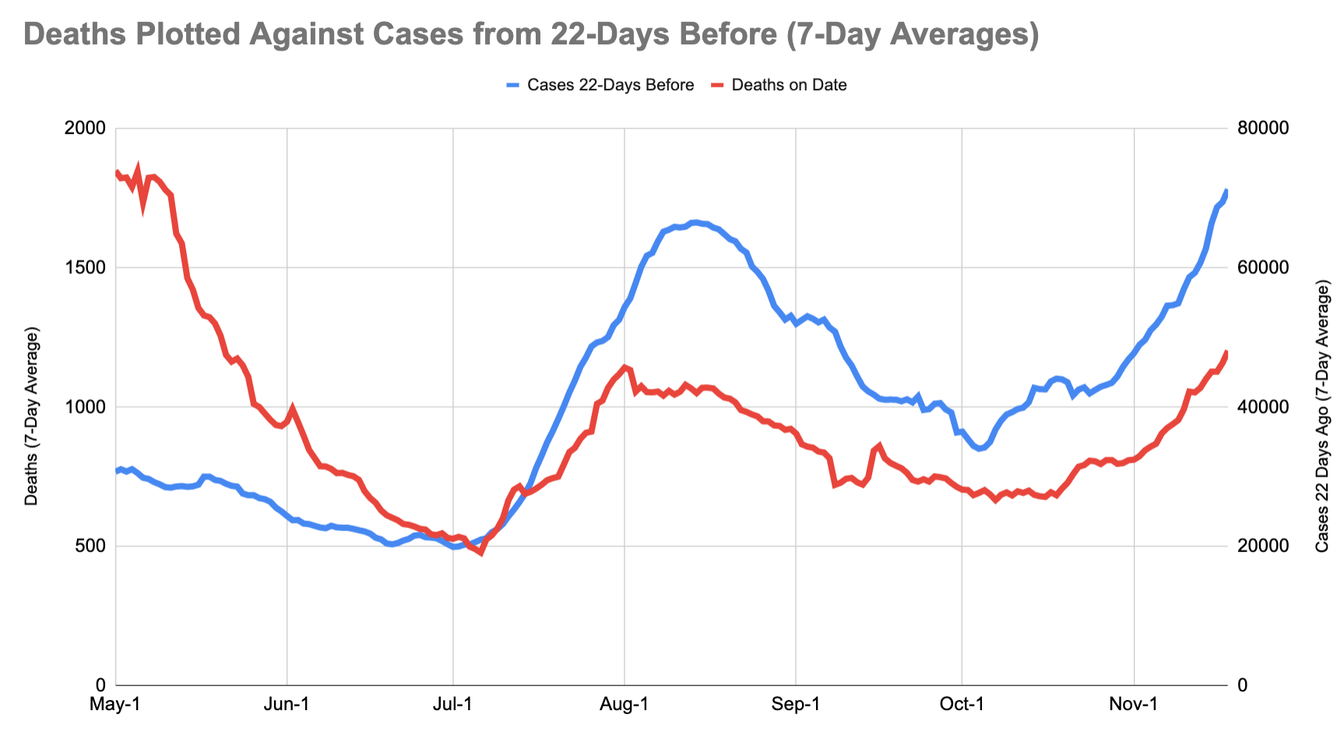
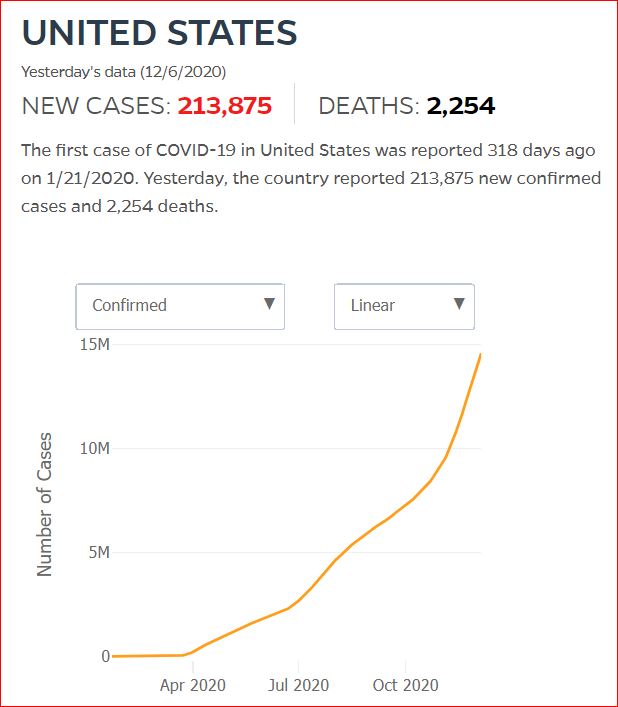
11/19/2020 How Many Americans Are About to Die? by Alexis D. Madrigal and Whet Moser, The Atlantic
A new analysis shows that the country is on track to pass spring’s grimmest record.
The chart you're looking at is as simple as it is disturbing. It shows that, as we should expect, far fewer people are dying, per reported cases, than in the early days of the pandemic. But on the chart below, look at August, where much of the published research on death rates ends. The improvement stops.
The numbers in the first week of August are not much different from the numbers in the first week of November. By Bedford’s method, the lagged case-fatality rate has averaged 1.8 percent since August.
This should be an extremely urgent signal that the U.S. response to COVID-19 has put the country on a dangerous track.
- These estimates were prepared by Trevor Bedford, a genomic epidemiologist at the Fred Hutchinson Cancer Research Center, in Seattle, using data from the COVID Tracking Project at The Atlantic, which compiles the cases and deaths that states report. They were then independently analyzed by the forecasting expert Ryan Tibshirani at the Delphi Group at Carnegie Mellon, which works closely with the CDC on disease modeling. If we look back over the past several months, the method Bedford used has proved more accurate than other means of forecasting near-term deaths.


12/22/2020 A primer on paradox in medical test statistics, specificity, sensitivity, true and false positive and negative rates, odds vs probability, Prevalence, Prior, and Bayes, Oh my!
June 28: Yes, you should still go to the dentist. But be careful, by Teddy Amenabar, The Washington Post
The CDC reports there’s “no data available to assess the risk of SARS-CoV-2 transmission during dental practice.”
Science: Reducing transmission of SARS-CoV-2, Kimberly A. Prather, Chia C. Wang, Robert T. Schooley, 5/27/2020
The World Health Organization (WHO) recommendations for social distancing of 6 ft and hand washing to reduce the spread of SARS-CoV-2 are based on studies of respiratory droplets carried out in the 1930s. These studies showed that large, ~100 μm droplets produced in coughs and sneezes quickly underwent gravitational settling (1). However, when these studies were conducted, the technology did not exist for detecting submicron aerosols.
As a comparison, calculations predict that in still air, a 100-μm droplet will settle to the ground from 8 ft in 4.6 s whereas a 1-μm aerosol particle will take 12.4 hours (4). Measurements now show that intense coughs and sneezes that propel larger droplets more than 20 ft can also create thousands of aerosols that can travel even further (1). Increasing evidence for SARS-CoV-2 suggests the 6 ft WHO recommendation is likely not enough under many indoor conditions where aerosols can remain airborne for hours, accumulate over time, and follow air flows over distances further than 6 ft (5, 10).
Traditional respiratory disease control measures are designed to reduce transmission by droplets produced in the sneezes and coughs of infected individuals. However, a large proportion of the spread of coronavirus disease 2019 (COVID-19) appears to be occurring through airborne transmission of aerosols produced by asymptomatic individuals during breathing and speaking (1–3). Aerosols can accumulate, remain infectious in indoor air for hours, and be easily inhaled deep into the lungs. For society to resume, measures designed to reduce aerosol transmission must be implemented, including universal masking and regular, widespread testing to identify and isolate infected asymptomatic individuals
Washington Post: Virus ‘does not spread easily’ from contaminated surfaces or animals, revised CDC website states, by Ben Guarino and Joel Achenbach, 5/21/2020
SciTechDaily: Yikes! Saliva Droplets From Mild Cough Travel Up to 18 Feet, Talib Dbouk and Dimitris Drikakis, Physics of Fluids, 5/19/2020
Physics of Fluids: On coughing and airborne droplet transmission to humans, by Talib Dbouk and Dimitris Drikakis, 5/19/2020
New York Times: Talking Can Generate Coronavirus Droplets That Linger Up to 14 Minutes, by Knvul Sheikh, 5/14/2020
Coughs or sneezes may not be the only way people transmit infectious pathogens like the novel coronavirus to one another. Talking can also launch thousands of droplets so small they can remain suspended in the air for eight to 14 minutes, according to a new study.
PNAS: The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission, by Valentyn Stadnytskyi, Christina E. Bax, Adriaan Bax and Philip Anfinrud, 5/13/2020
Highly sensitive laser light scattering observations have revealed that loud speech can emit thousands of oral fluid droplets per second. In a closed, stagnant air environment, they disappear from the window of view with time constants in the range of 8 to 14 min, which corresponds to droplet nuclei of ca. 4 μm diameter, or 12- to 21-μm droplets prior to dehydration. These observations confirm that there is a substantial probability that normal speaking causes airborne virus transmission in confined environments.
Daily Beast: Can You Spread the Virus Just by Speaking?, by David Axe, 4/20/2020
The virus that causes COVID-19 could be a lot easier to spread than many people realize. It might even be possible to give somebody the SARS-CoV-2 virus by simply talking to them, a team of scientists concluded.
New England Journal of Medicine: Visualizing Speech-Generated Oral Fluid Droplets with Laser Light Scattering, by Philip Anfinrud, Valentyn Stadnyskyi (NIH) and Christina E. Bax (Penn)
The act of speaking generates oral fluid droplets that vary widely in size,1 and these droplets can harbor infectious virus particles. Whereas large droplets fall quickly to the ground, small droplets can dehydrate and linger as “droplet nuclei” in the air, where they behave like an aerosol and thereby expand the spatial extent of emitted infectious particles.2 We report the results of a laser light-scattering experiment in which speech-generated droplets and their trajectories were visualized.
CNN: Experts tell White House coronavirus can spread through talking or even just breathing, By Elizabeth Cohen,4/2/2020
Medium: Hold the Line. This virus is unforgiving to unwise choices, by Jonathan Smith, 3/20/2020
"As an infectious disease epidemiologist (albeit a junior one), I feel morally obligated to provide information on what we are seeing from a transmission dynamic perspective and how it applies to the social distancing measures. Like any good scientist, I have noticed two things that are either not well articulated or not present in the “literature” of online media. I have also relied on other infectious disease epidemiologists for peer review of this piece.
Specifically, I want to make two aspects of these distancing measures very clear and unambiguous.
First, we are in the very infancy of this epidemic’s trajectory. That means that even with these measures in place, we will see cases and deaths continue to rise globally, nationally, and in our own communities. This may lead some to think that the social distancing measures are not working. They are. They may feel futile. They aren’t. You will feel discouraged. You should. This is normal in chaos. This is the normal epidemic trajectory. Stay calm.
The enemy we are facing is very good at what it does; we are not failing. We need everyone to hold the line as the epidemic inevitably gets worse. This is not an opinion. This is the unforgiving math of epidemics for which I and my colleagues have dedicated our lives to understanding with great nuance, and this disease is no exception. Stay strong and in solidarity knowing that what you are doing is saving lives, even as people continue getting sick and dying. You may feel like giving in. Don’t.
You should perceive your entire family to function as a single individual unit: if one person puts themselves at risk, everyone in the unit is at risk.
Second, although social distancing measures have been (at least temporarily) well received, there is an obvious-but-overlooked phenomenon when considering groups (i.e. households) in transmission dynamics. While social distancing decreases contact with members of society, it of course increases contact within a group (i.e. family). This small and obvious fact has surprisingly profound implications on disease transmission dynamics. The basic mechanics of this mathematical principle dictate that even if there is only a little bit of additional connection between groups (i.e. social dinners, playdates, unnecessary trips to the store, etc.), the epidemic likely won’t be much different than if there was no measure in place. The same underlying fundamentals of disease transmission apply, and the result is that the community is left with all of the social and economic disruption but very little public health benefit.
You should perceive your entire family to function as a single individual unit: If one person puts themselves at risk, everyone in the unit is at risk. Seemingly small social chains get large and complex with alarming speed. If your son visits his girlfriend, and you later sneak over for coffee with a neighbor, your neighbor is now connected to the infected office worker that your son’s girlfriend’s mother shook hands with. This sounds silly, it’s not. This is not a joke or hypothetical. We as epidemiologists see it borne out in the data time and time again. Conversely, any break in that chain breaks disease transmission along that chain.
In contrast to hand-washing and other personal measures, social distancing measures are not about individuals, they are about societies working in unison. These measures also require sustained action before results are evident. It is hard (even for me) to conceptualize how on a population level ‘one quick little get together’ can undermine the entire framework of a public health intervention, but it can. I promise you it can. I promise. I promise. I promise. You can’t cheat it. People are already itching to cheat on the social distancing precautions just a “little”- a short playdate, a quick haircut, or picking up a needless item from the store. From a transmission dynamics standpoint, this very quickly recreates a highly connected social network that undermines much of the good work our communities have done thus far.
This outbreak will not be overcome in one grand, sweeping gesture, but rather by the collection of individual choices we make in the coming months. This virus is unforgiving to unwise choices. As this epidemic continues, it will be easy to be drawn to the idea that what we are doing isn’t working and we may feel compelled to “cheat” with unnecessary breaches of social distancing measures. By knowing what to expect, and knowing the critical importance of maintaining these measures, my hope is to encourage continued community spirit and strategizing to persevere in this time of uncertainty."
Jonathan Smith is an infectious disease epidemiologist focusing on the dynamics of disease transmission. PhD en route at Emory, Lecturer at Yale.
Youtube: Ninja Nerd: Epidemics and the coronavirus infection, the ARDS and pneumonia timeline explained. 3/16/2020
Youtube: Ninja Nerd: COVID-19 | Corona Virus: Treatment, Prognosis, Precautions, 3/18/2020
March 1, 2020: US Surgeon General: Face masks won't protect from coronavirus, stop buying them, by Stefanie Dyga, Mid-Michigan NOW
Updated 5/17/2020
6/16/2020: Children are only half as likely to get infected by the coronavirus, study finds, by Joel Achenbach and Laura Meckler, The Washington Post
Children and teenagers are only half as likely to get infected with the coronavirus as adults age 20 and older, and they usually don’t develop clinical symptoms of covid-19, the disease caused by the virus, according to a study published Tuesday.
6/16/2020: Age-dependent effects in the transmission and control of COVID-19 epidemics, by Nicholas G. Davies, Petra Klepac, Yang Liu, Kiesha Prem, Mark Jit, CMMID COVID-19 working group & Rosalind M. Eggo, Nature Medicine
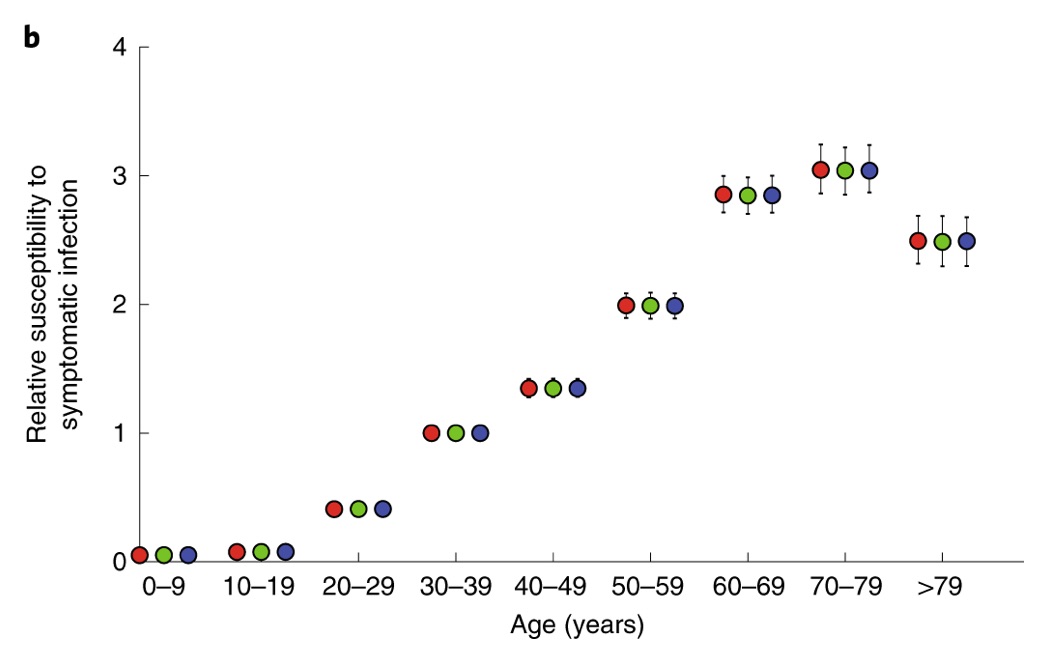
We estimate that susceptibility to infection in individuals under 20 years of age is approximately half that of adults aged over 20 years, and that clinical symptoms manifest in 21% (95% credible interval: 12–31%) of infections in 10- to 19-year-olds, rising to 69% (57–82%) of infections in people aged over 70 years.
LA Times: What’s the link between the coronavirus and the Kawasaki-like disease MIS-C?, by Deborah Netburn, 5/22/2020
Augusta University: Tiny RNA That Should Attack COVID-19 Coronavirus Diminish With Age, Disease, 5/17/2020
With age and some chronic medical conditions, the attacking microRNA numbers dwindle, reducing our ability to respond to viruses, says Dr. Carlos M. Isales, co-director of the MCG Center for Healthy Aging and chief of the MCG Division of Endocrinology, Diabetes and Metabolism.
Much like not having enough troops on the ground in an actual war, the coronavirus is then better able to do what it does naturally, which is hijack our cell machinery so it can replicate, say the researchers who report in the journal Aging and Disease what appear to be key microRNA involved in responding to this virus.
Aging and Disease: “COVID-19 Virulence in Aged Patients Might Be Impacted by the Host Cellular MicroRNAs Abundance/Profile” by Fulzele Sadanand, Sahay Bikash, Yusufu Ibrahim, Lee Tae Jin, Sharma Ashok, Kolhe Ravindra and Isales Carlos M, 13 May 2020
"in silico analysis"
New York Times: A New Coronavirus Threat to Children, by Pam Belluck, 5/11/2020
New York Times: Tiny RNA That Should Attack COVID-19 Coronavirus Diminish With Age, Disease, 5/13/2020
Twitter: The question of why children are mostly spared, Nicholas A. Christakis, M.D., 3/28/2020
https://twitter.com/NAChristakis/status/1243883141900763137?s=20
Let’s talk about the fact that both the attack rate and the death rate among the young is indeed very low with COVID19, unlike most prior pandemics. And let’s speculate about some of the biological reasons. 1/
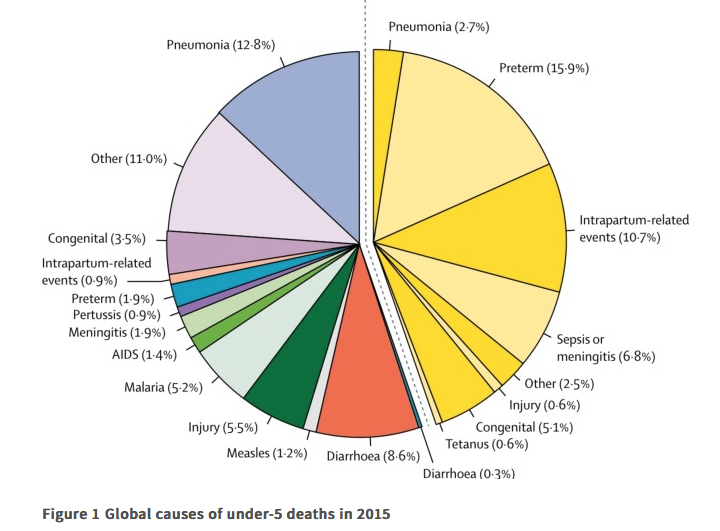
Kids suffer so much from infectious disease around the world. It’s their leading killer (https://thelancet.com/journals/lancet/article/PIIS0140-6736(16)31593-8/fulltext… ). And so I find it haunting and sweet that they might escape the predations of COVID19. 2/
Let’s define some terms. The “attack rate” is the probability that a person will come to be infected during an epidemic. Even for COVID19, it is unlikely to be >40% in the end (i.e., within the next three years); maybe just 20% of us will get it, eventually. 3/
The “infection fatality rate” (IFR) is the probability a person will die if infected. The “(symptomatic) case fatality rate” (sCFR or CFR) is the probability of death, given that one comes to medical attention (or has symptoms). 4/
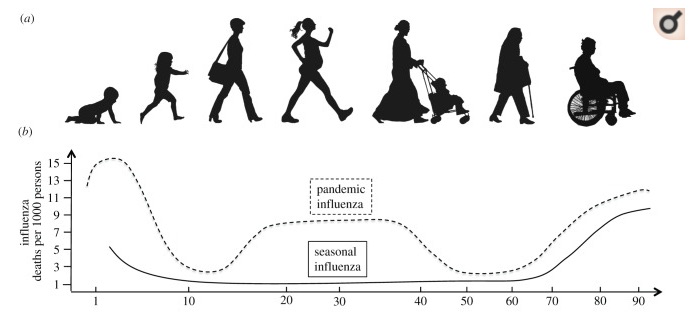
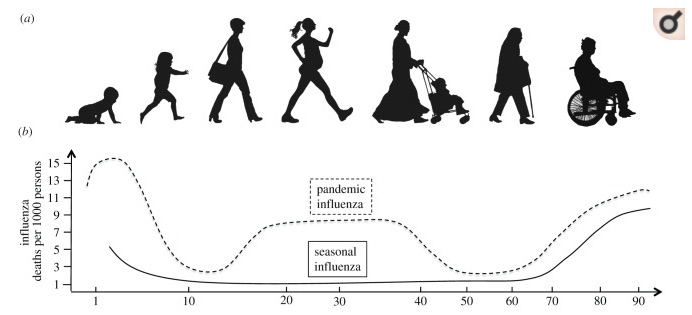
In most respiratory disease pandemics, both the very young and the very old are likely to die, resulting in a U-shaped function with age. The 1918 pandemic famously had a W-shaped function (where working-age adults also died). COVID19 is different: curve is flat at young ages. 5/
From early on, it was clear COVID19 spared children. In Wuhan, no children tested positive between November 2019 and mid-January, per an early report https://who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf… 6/
A study of 391 cases and 1,286 close contacts in Shenzhen, China, showed that kids under 9 had an attack rate of 7.4%, similar to adults (though adults 60-69 had a higher attack rate of 15.4%). https://medrxiv.org/content/10.1101/2020.03.03.20028423v2.full.pdf… 7/

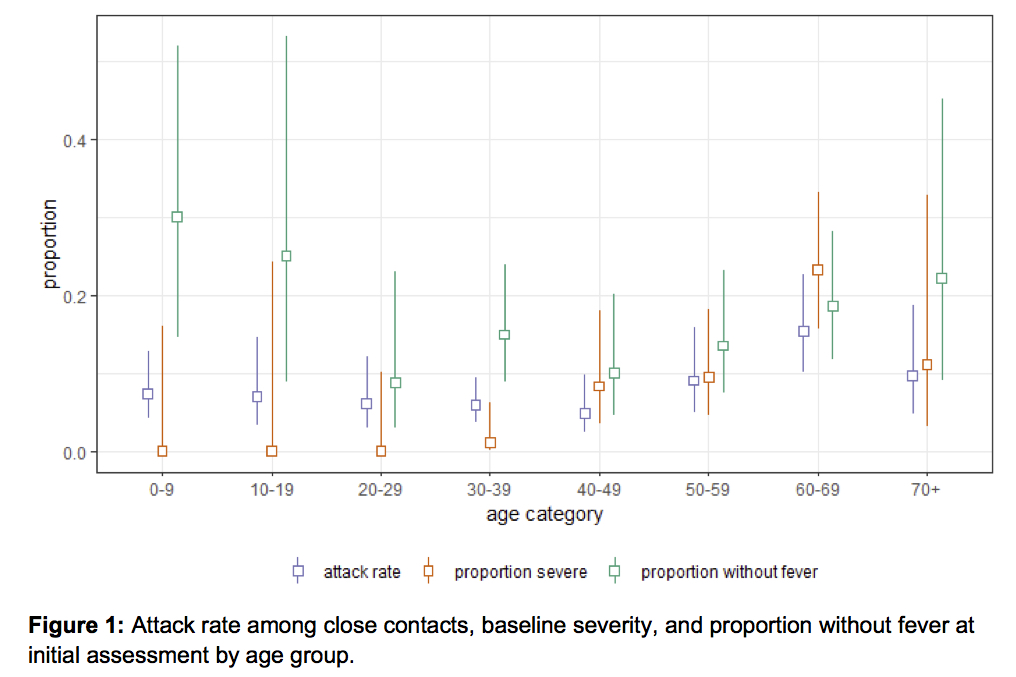
Overall, children were at a similar risk of infection as the adult population, though less likely to have severe symptoms, if infected. https://medrxiv.org/content/10.1101/2020.03.03.20028423v2.full.pdf… 8/
Another sophisticated study using multiple sources of data concluded that, compared to those aged 30–59 years, those aged <30 years and >59 years are 0.16 and 2.0 times more susceptible to symptomatic infection. https://nature.com/articles/s41591-020-0822-7… 9/
In other good news, transmission from pregnant women to their children in utero (known as ‘vertical transmission’) seems rare for COVID-19, too. https://jamanetwork.com/journals/jama/fullarticle/2763853… This is similar for SARS (from 2003). https://who.int/csr/sars/en/WHOconsensus.pdf… 10/
Not only is the ‘attack rate’ low in children (which we will need to confirm, eventually, with 'serological' tests in large random samples, as per: https://twitter.com/NAChristakis/status/1240689935557865472?s=20…), but the fatality rate, among those kids who do get infected, is VERY low. Yay! 11/
In Wuhan, China, a very small proportion of those aged under 19 years developed severe (2.5%) or critical disease (0.2%), an early study showed. https://who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf… 12/
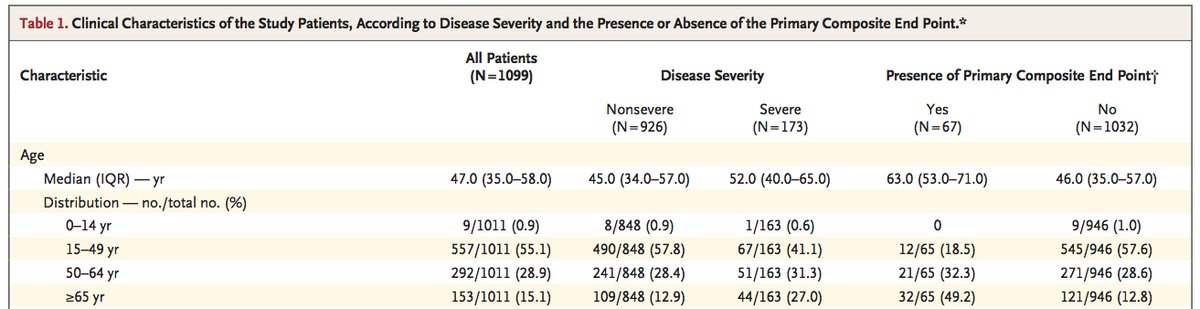
In a study of 1,099 patients in China, just 0.9 percent of confirmed cases were <14, and none died. https://nejm.org/doi/full/10.1056/NEJMoa2002032… 13/
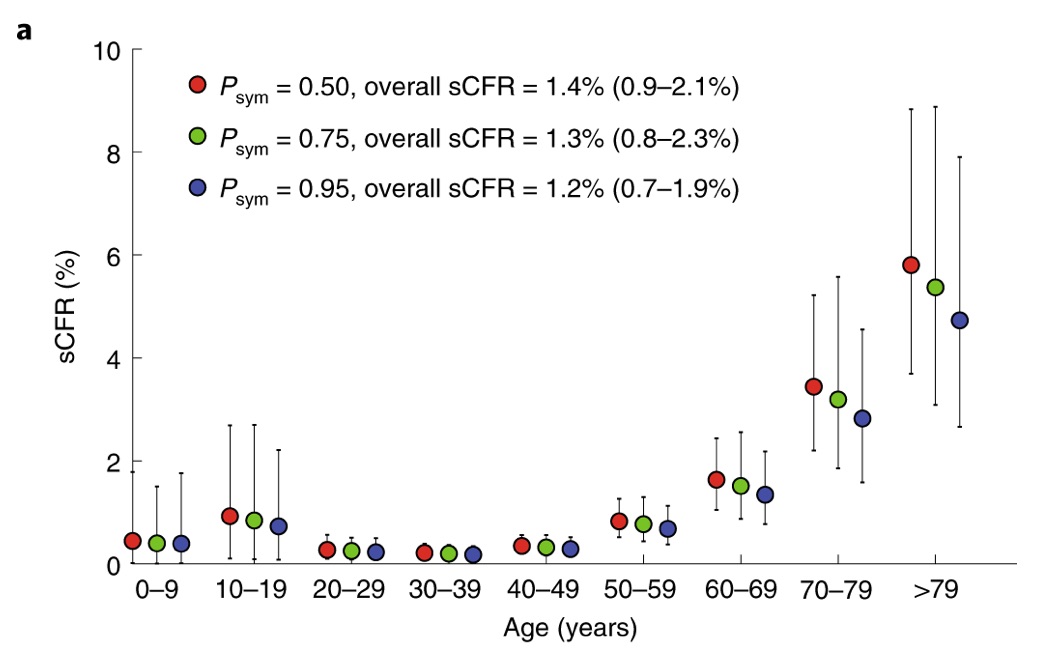
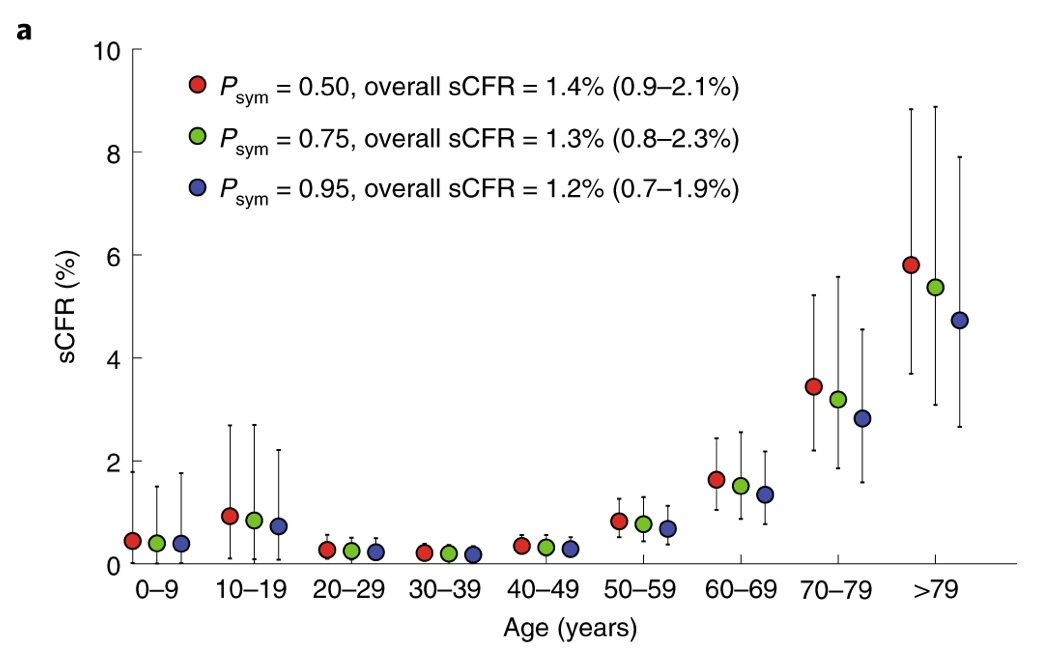
Another sophisticated study (cited above, too), using multiple sources of data https://nature.com/articles/s41591-020-0822-7…, found that, if probability of developing symptoms after infection, Psym, is 0.5, the sCFR values are 0.3% (aged <30 years), 0.5% (30–59 yrs) and 2.6% (>59 yrs). 14/
In the Diamond Princess cruise ship, there were 3,711 people and 634 cases of COVID19 (an attack rate of 17%). Half were asymptomatic. There were just 39 people <19 years old; only 5 got infected and only 2 had symptoms; and none died. https://medrxiv.org/content/10.1101/2020.03.05.20031773v2… 15/
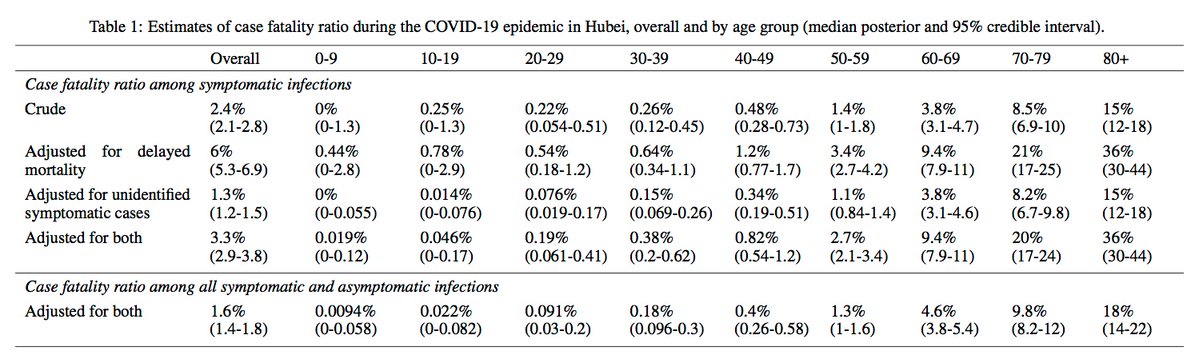
So, a sophisticated summary of COVID19 fatality in both symptomatic & asymptomatic patients (via https://medrxiv.org/content/10.1101/2020.03.04.20031104v1.full.pdf… ) is:
- Age 0-9: 0.0094%
- Age 10-19: 0.022%
- Age 20-29: 0.091%
- Age 30-39: 0.18%
- Age 40-49: 0.4%
- Age 50-59: 1.3%
- Age 60-69: 4.6%
- Age 70-79: 9.8%
- Age 80+: 18%
16/
But the best study to date (via American Academy of Pediatricians) – of 2,143 pediatric patients in China – found that, while 90% had mild or moderate illness, children <1 are indeed more likely to have critical illness, if infected. https://pediatrics.aappublications.org/content/pediatrics/early/2020/03/16/peds.2020-0702.full.pdf… 17/
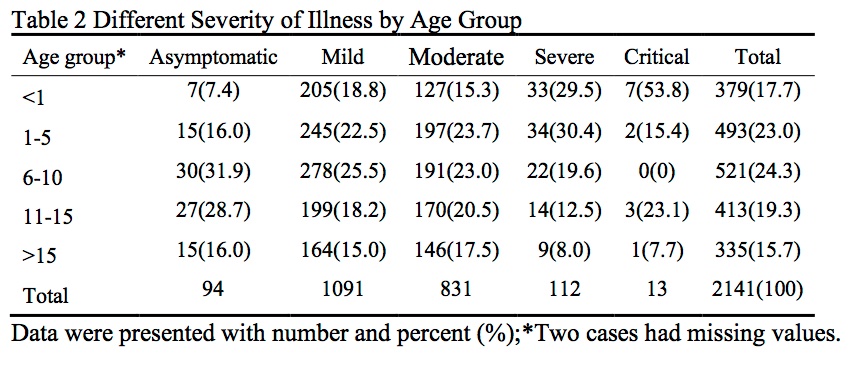
Yet, just one child out of the 2,143 in this large Chinese pediatric cohort (who was age 14), actually died. So death among kids with COVID19 is indeed *very* rare. https://nytimes.com/2020/03/17/health/coronavirus-childen.html… 18/
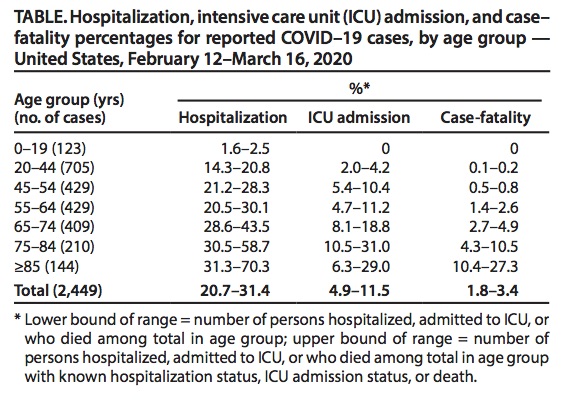
In the USA, as of March 18, a similar age-pattern for COVID19 was observed by the CDC. Among 2,449 cases, with 123 below age 19, there were no deaths in that young age group. https://cdc.gov/mmwr/volumes/69/wr/mm6912e2.htm… 19/
Something similar, in terms of relatively benign course in kids, was observed in the 2003 SARS pandemic (a similar, albeit much more deadly, pathogen – CFR of ~10%), as well. In Hong Kong, no one <24 years died but >50% of patients >65 died. https://who.int/csr/sars/en/WHOconsensus.pdf… (Table 3) 20/
Of course, with 100,000’s of people infected in USA, there will be some cases of young people dying. And they will get news coverage. 21/
The total US population of people <24 is about 104,000,000. With an attack rate of 7.4% and a CFR of ~0.04%, this means that about 3,000 young Americans will die of COVID19. 22/
But, even if death from COVID19 is rare for kids, they will be badly affected by our *responses* to the COVID19 pandemic -- which involve unemployment, dislocation, and fear -- as this fine essay in The Atlantic argues: https://theatlantic.com/health/archive/2020/03/what-coronavirus-will-do-kids/608608/… Kids suffer in disasters. 23/
To be clear, kids can indeed *transmit* the disease, which one reason (of several) that school closures are an effective tool for tamping down on the COVID19 epidemic. The little vectors. https://twitter.com/NAChristakis/status/1235204443362205699?s=20… 24/
There are a number of possible biological explanations for kids’ relative lack of sensitivity to COVID-19: https://the-scientist.com/news-opinion/possible-biological-explanations-for-kids-escape-from-covid-19-67273… Immunologists and pediatricians have many ideas, but we just don’t know for sure yet. [thread continues...] 25/
One idea is that children have more “adaptive” immunity (optimized for pathogens they have *not* previously seen) and that adults have more “memory” driven immunity (geared to pathogens they have indeed seen before). 26/
Another idea, is that past immunity to *other* coronaviruses might make COVID19 worse for adults by an immunological *over-reaction* to a novel coronavirus. A lot of COVID19 morbidity may be due, actually, to our bodies overreacting to the virus. 27/,
Or could it be that “ACE2 receptors” (a protein on our cells that the virus binds to) are more immature in the lungs of the young, and so they provide less of a target for SARS-CoV-2 to enter our cells (I think this unlikely). 28/
Another idea relates to the aging lung environment. In order for individuals not to overreact to irritants, aged lungs counter the usual immune reaction with some tamping down of inflammation. https://the-scientist.com/news-opinion/possible-biological-explanations-for-kids-escape-from-covid-19-67273… 29/
Children may have more efficient CD4+ helper T cells which stimulate B cells to make antibodies against pathogens. Possibly, the type of T cell that dominates early in life is better at repelling SARS-CoV-2. https://the-scientist.com/news-opinion/possible-biological-explanations-for-kids-escape-from-covid-19-67273… 30/
So there are lots of ideas about why kids might be spared. We need more SCIENCE. But this much is already clear: kids are somewhat less likely to be infected with SARS-CoV-2 and substantially less likely to get seriously ill if infected. 31/
Regarding the variation in our immune system with age, see: https://ncbi.nlm.nih.gov/pmc/articles/PMC4707740/pdf/rspb20143085.pdf… 32/
I need to note that, despite my delight that the young are spared in this pandemic, this does not mean that it’s no big deal that the elderly die! I’ve been very upset by the narrative that ‘it’s just old folks.’ We are speaking of our parents, grandparents, and neighbors! 33/
In the end, what will probably happen is that SARS-CoV-2 will become “endemic” (it will always circulate in our species and we’ll get used to it). Once kids are immunized by being exposed, they will not get as sick from it once they grow up to be the adults of tomorrow. 34/
9/

Michigan COVID-19 Test Finder
Michigan coronavirus cases: Tracking the pandemic, by Pat Byrne, Brian McNamara, Brian Todd, and Kristi Tanner, Detroit Free Press
Data, Charts, Graphs, Trends, Demographics
91-DIVOC: An interactive visualization of the exponential spread of COVID-19, Fascinating and interactive.
91-DIVOC: COVID-19 Data for Locations of People You Love (Washtenaw County, for example)
Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU)
The Lancet COVID-19 Resource Center - free
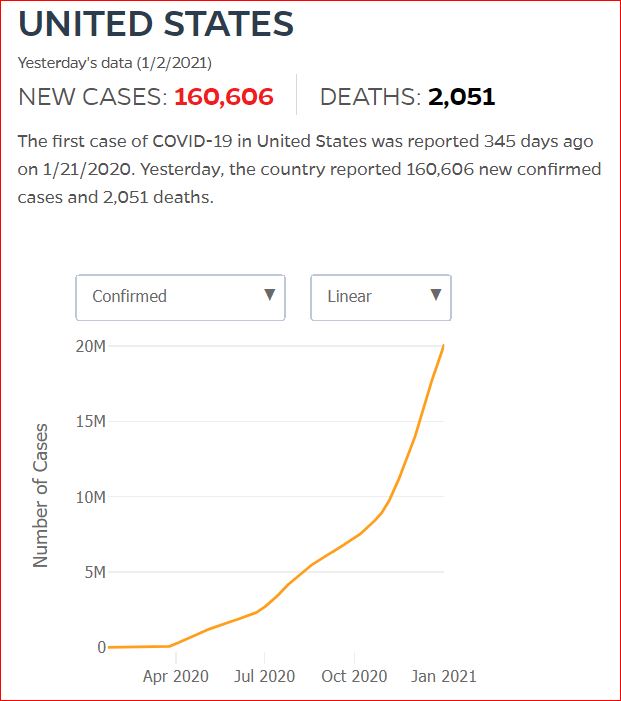
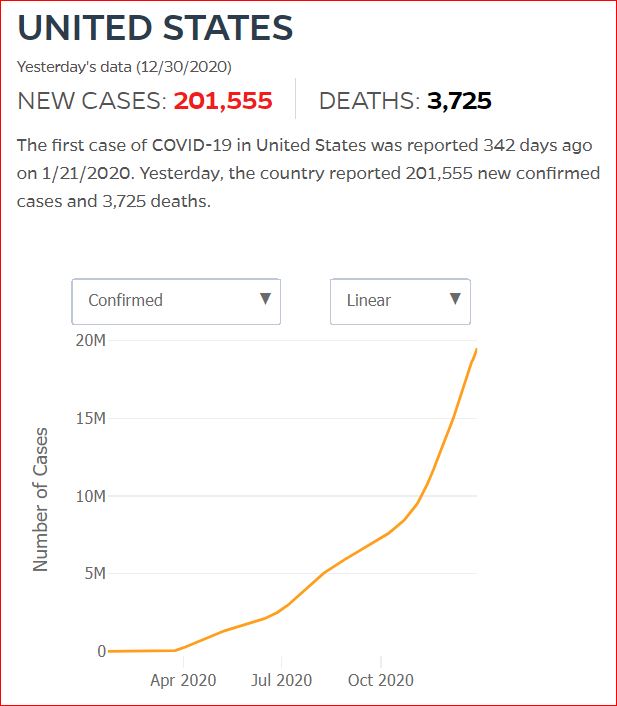
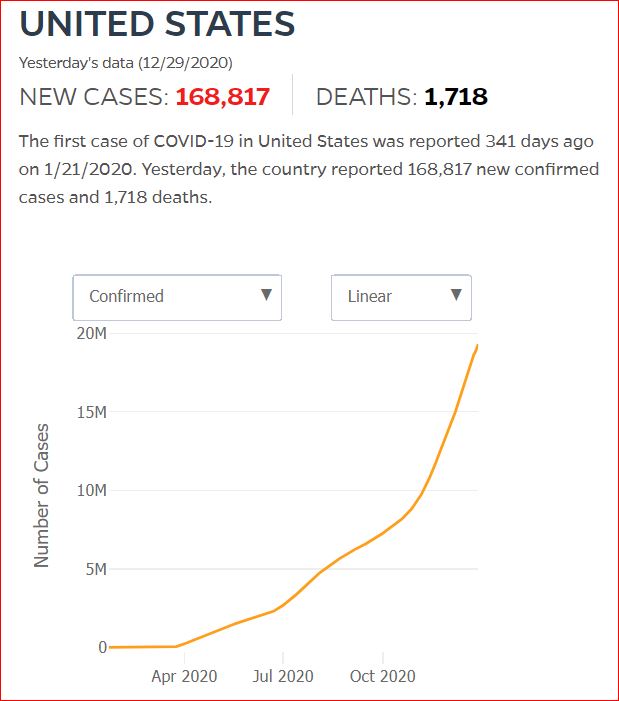
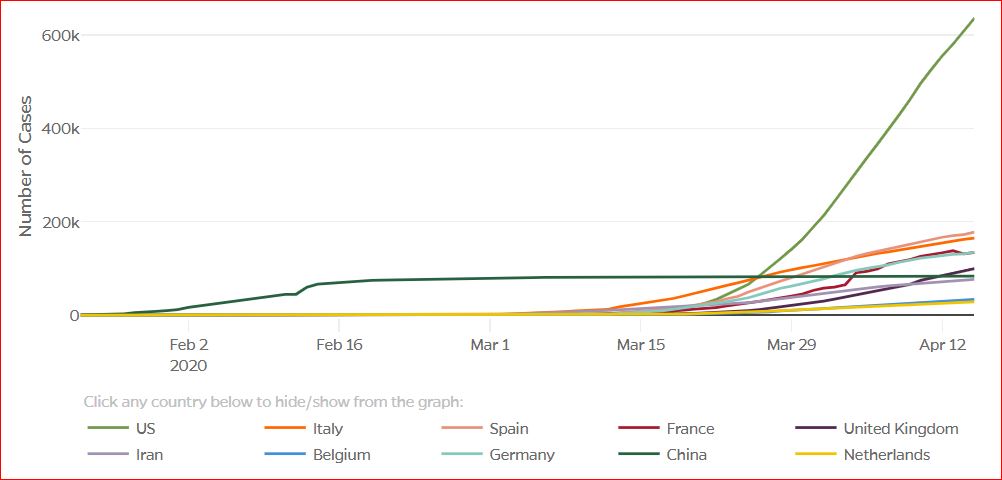
Cumulative Cases - Johns Hopkins University - updated every day, sometimes at about 3:00 AM, sometimes later.
USA Facts: US Coronavirus Cases and Deaths: Track COVID-19 data daily by state and county
This interactive feature aggregates data from the Centers for Disease Control and Prevention (CDC), state- and local-level public health agencies. County-level data is confirmed by referencing state and local agencies directly. Cases, deaths, and per capita adjustments reflect cumulative totals since January 22, 2020.
Detailed Methodology and Sources: COVID-19 Data
Detailed methodology on how USAFacts collects COVID-19 dataPublished on Fri, April 24, 2020 12:00AM PDT | Updated Wed, July 8, 2020 4:38PM PDT
USA Facts: Coronavirus Stats & Data - this data source was funded by Microsoft cofounder Steve Ballmer
12/22/2020 A primer on paradox in medical test statistics, specificity, sensitivity, true and false positive and negative rates, odds vs probability, Prevalence, Prior, and Bayes, Oh my!
10/9/2020 The Coronavirus Unveiled, by Carl Zimmer, The New York Times (computational virology illustrated)
Sept 24, 2020 Modeling between-population variation in COVID-19 dynamics in Hubei, Lombardy, and New York City, by Bryan Wilder, Marie Charpignon, Jackson A. Killian, Han-Ching Ou, Aditya Mate, Shahin Jabbari, Andrew Perrault, Angel N. Desai, Milind Tambe, and Maimuna S. Majumder, PNAS
Sept 9, 2020 Demographic perspectives on the mortality of COVID-19 and other epidemics by Joshua R. Goldstein and Ronald D. Lee, PNAS
To put estimates of COVID-19 mortality into perspective, we estimate age-specific mortality for an epidemic claiming for illustrative purposes 1 million US lives, with results approximately scalable over a broad range of deaths. We calculate the impact on period life expectancy (down 2.94 y) and remaining life years (11.7 y per death). Avoiding 1.75 million deaths or 20.5 trillion person years of life lost would be valued at $10.2 to $17.5 trillion. The age patterns of COVID-19 mortality in other countries are quite similar and increase at rates close to each country’s rate for all-cause mortality. The scenario of 1 million COVID-19 deaths is similar in scale to that of the decades-long HIV/AIDS and opioid-overdose epidemics but considerably smaller than that of the Spanish flu of 1918. Unlike HIV/AIDS and opioid epidemics, the COVID-19 deaths are concentrated in a period of months rather than spread out over decades.
July 28, 2020 Tracking the reach of COVID-19 kin loss with a bereavement multiplier applied to the United States, by Ashton M. Verdery, Emily Smith-Greenaway, Rachel Margolis and Jonathan Daw, PNAS
COVID-19 has created a mortality shock throughout the world, and it may yield a second wave of population health concerns tied to bereavement and social support reductions. We created the COVID-19 bereavement multiplier, an indicator that clarifies one downstream impact of COVID-19 mortality and can be applied to different epidemiological projections of death counts: How many people are at risk for losing a grandparent, parent, sibling, spouse, or child for each COVID-19 death. In the United States, we estimate that on average, under diverse epidemiological circumstances, every death from COVID-19 will leave approximately nine bereaved. Studying how acute mortality crises reverberate through a population in the form of bereavement multipliers expands understandings of the social impacts of health crises.
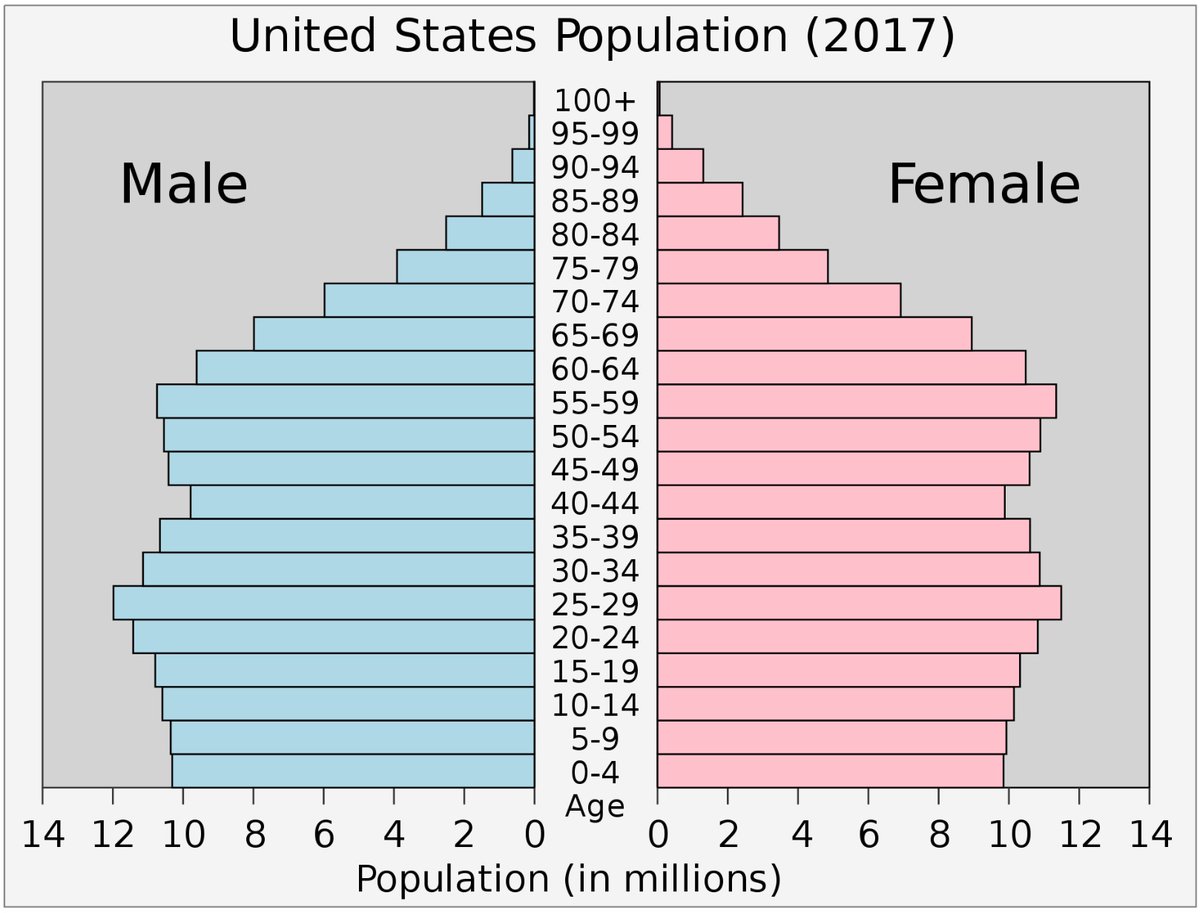
July 14, 2020 National age and coresidence patterns shape COVID-19 vulnerability, by Albert Esteve, Iñaki Permanyer, Diederik Boertien, and James W. Vaupel, PNAS
April 21, 2020 Projecting hospital utilization during the COVID-19 outbreaks in the United States, by Seyed M. Moghadas, Affan Shoukat, Meagan C. Fitzpatrick, Chad R. Wells, Pratha Sah, Abhishek Pandey, Jeffrey D. Sachs, Zheng Wang, Lauren A. Meyers, Burton H. Singer, and Alison P. Galvani
March 31, 2020 IMpact of international travel and border control measures on the global spread of the novel 2019 coronavirus outbreak, by Chad R. Wells, Pratha Sah, Seyed M. Moghadas, Abhishek Pandey, Affan Shoukat, Yaning Wang, Zheng Wang, Lauren A. Meyers, Burton H. Singer, and Alison P. Galvani, PNAS
To contain the global spread of the 2019 novel coronavirus epidemic (COVID-19), border control measures, such as airport screening and travel restrictions, have been implemented in several countries. Our results show that these measures likely slowed the rate of exportation from mainland China to other countries, but are insufficient to contain the global spread of COVID-19. With most cases arriving during the asymptomatic incubation period, our results suggest that rapid contact tracing is essential both within the epicenter and at importation sites to limit human-to-human transmission outside of mainland China.
The novel coronavirus outbreak (COVID-19) in mainland China has rapidly spread across the globe. Within 2 mo since the outbreak was first reported on December 31, 2019, a total of 566 Severe Acute Respiratory Syndrome (SARS CoV-2) cases have been confirmed in 26 other countries. Travel restrictions and border control measures have been enforced in China and other countries to limit the spread of the outbreak. We estimate the impact of these control measures and investigate the role of the airport travel network on the global spread of the COVID-19 outbreak. Our results show that the daily risk of exporting at least a single SARS CoV-2 case from mainland China via international travel exceeded 95% on January 13, 2020. We found that 779 cases (95% CI: 632 to 967) would have been exported by February 15, 2020 without any border or travel restrictions and that the travel lockdowns enforced by the Chinese government averted 70.5% (95% CI: 68.8 to 72.0%) of these cases. In addition, during the first three and a half weeks of implementation, the travel restrictions decreased the daily rate of exportation by 81.3% (95% CI: 80.5 to 82.1%), on average. At this early stage of the epidemic, reduction in the rate of exportation could delay the importation of cases into cities unaffected by the COVID-19 outbreak, buying time to coordinate an appropriate public health response.
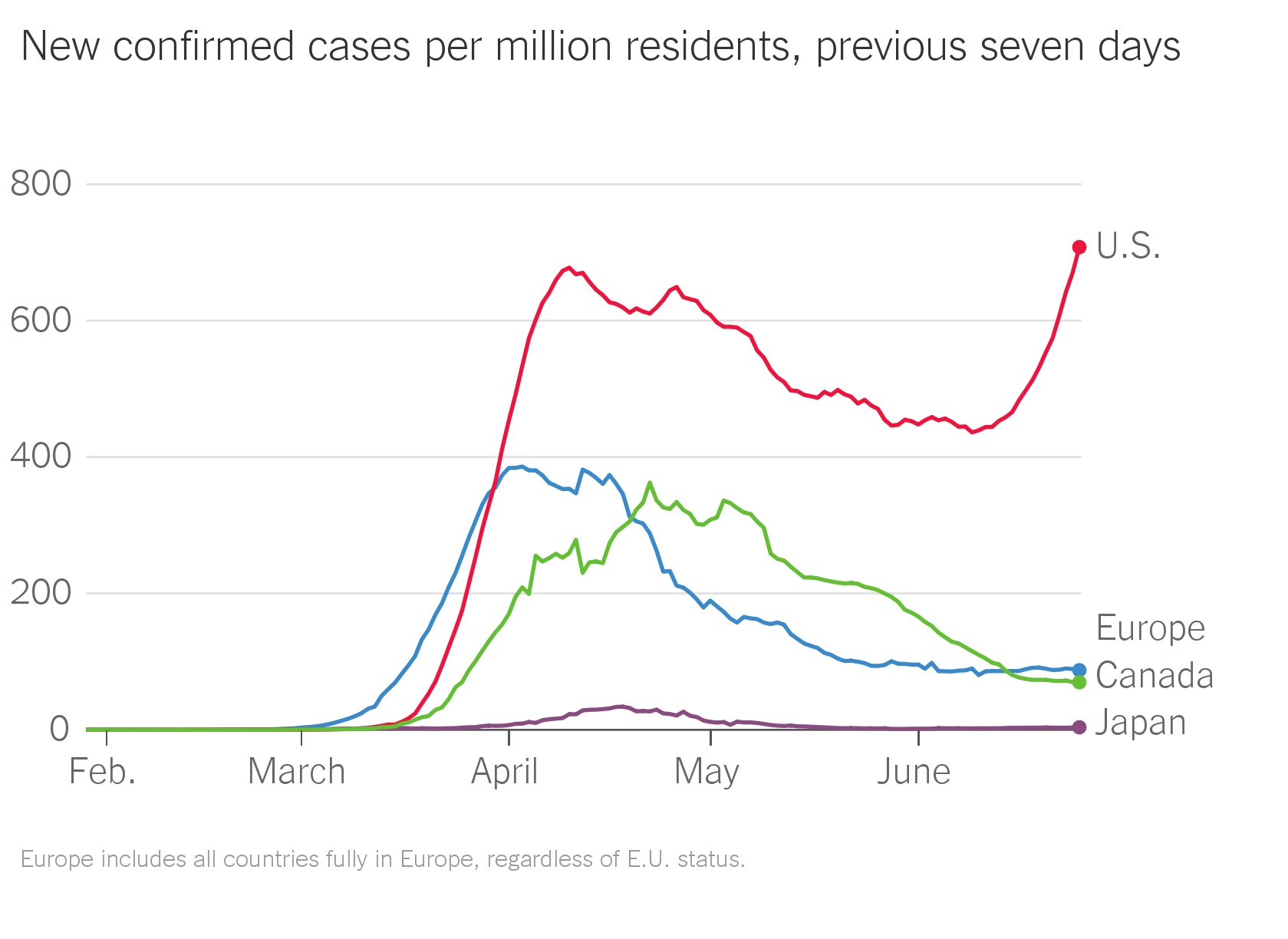
June 29, 2020. American Exceptionalism on the Virus.
The 9/11 death toll was 2,977 people.
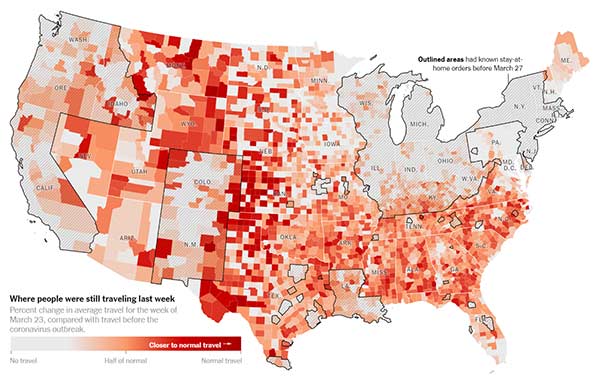
The New York Times: Where America Didn’t Stay Home Even as the Virus Spread, By James Glanz, Benedict Carey, Josh Holder, Derek Watkins, Jennifer Valentino-DeVries, Rick Rojas and Lauren Leatherby, April 2, 2020
Florida waited so long to shut down travel that it will struggle to control local outbreaks even if people immediately change their behavior significantly, said Thomas Hladish, an infectious disease modeler at the University of Florida. People who now sequester themselves at home still risk having brought the virus home to their families, he said.
"A lockdown order right now is not going to be a silver bullet with containing this," Mr. Hladish said. "It will absolutely save lives. But in order to really have a big effect with social-distancing measures, you would have had to move it back in time.”
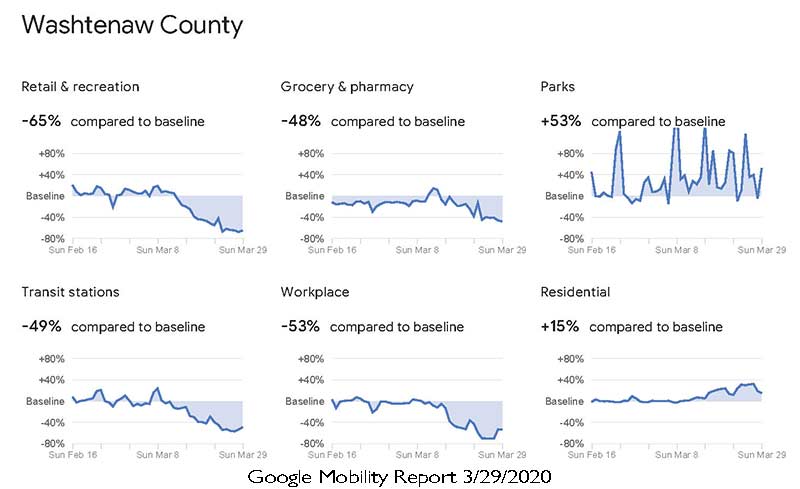
The Verge: Google uses location data to show which places are complying with stay-at-home orders — and which aren’t, by Casey Newton, 4/3/2020
New COVID-19 mobility reports show changes in traffic to stores, parks, transit stations, and more.
Google: Community Mobility Reports 3/29/2020 is the current update
Google: State of Michigan COVID-19 Mobility Report
Statistics Trackers:
Washtenaw County Health Department: COVID-19 Cases in Washtenaw County Updated 4/4/2020
Michigan.Gov statistics, updated daily at 2pm:
CDC: COVID-10: U.S. at a Glance
Worldometers.info Worldometer's COVID-19 data
Detroit Free Press: Michigan coronavirus cases: Tracking the pandemic, 4/17/2020
nCoV2019.live
C19 Coronavirus Statistics
Statnews.com A Covid-19 data tracker
- Click on a country name to get a more detailed geographic breakdown at the state, province, or county level.
The COVID Tracking Project
CNN: More than 150 employees at 4 Boston hospitals have tested positive for coronavirus, Jason Hanna and Ellie Kaufman, 3/27/2020
CNN: Italy records highest daily jump in coronavirus deaths, Sara Spary, Valentina DiDonato, Sharon Braithwaite, 3/27/2020
The number of people who have died of novel coronavirus in Italy has risen by 969 in the past day, the biggest daily jump since the crisis began.
BBC: Coronavirus: A visual guide to the economic impact, Lora Jones, David Brown & Daniele Palumbo, 3/27/2020
MLive: Michigan confirms new coronavirus cases, raising total to 65. Coronavirus is being found in residents across the state, but Wayne County has the most cases of any Michigan county so far, with 17 total. - Malachi Barrett, 3/17/2020
Washington Post - 1/31/2020 Days Events reports
https://www.cnn.com/asia/live-news/coronavirus-outbreak-01-31-20-intl-hnk/index.html

Photo by Dr. Frederick A. Murphy
You call a friend and arrange to meet for lunch. It’s unseasonably springlike, so you choose a place with outdoor seating, which seems like it should be safer. As usual, you take all reasonable precautions: You use hand sanitizer, sit a good distance from other customers, and try to avoid touching your face, though that last part is hard. A part of you suspects that this whole thing might be overblown.
What you don’t know is that ten days ago, your friend’s father was a guest of his business partner at the University Club, where he caught the novel coronavirus from the wife of a cryptocurrency speculator. Three days after that, he coughed into his hand before opening the door of his apartment to welcome his son home. The saliva of COVID-19 patients can harbor half a trillion virus particles per teaspoon, and a cough aerosolizes it into a diffuse mist. As your friend walked through the door he took a breath and 32,456 virus particles settled onto the lining of his mouth and throat.
Viruses have been multiplying inside his body ever since. And as he talks, the passage of his breath over the moist lining of his upper throat creates tiny droplets of virus-laden mucus that waft invisibly into the air over your table. Some settle on the as-yet-uneaten food on your plate, some drift onto your fingers, others are drawn into your nasal sinus or settle into your throat. By the time you extend your hand to shake good-bye, your body is carrying 43,654 virus particles. By the time you’re done shaking hands, that number is up to 312,405.
Read more of this here: New York Magazine: How the Coronavirus Could Take Over Your Body (Before You Ever Feel It) by Jeff Wise, 3/18/2020.
1/14/2021 The Coronavirus Is Mutating. Here’s What We Know, Wall Street Journal Video
1/12/2021 The Future of the Coronavirus? An Annoying Childhood Infection, by Apoorva Mandavilli, The New York Times
As millions are inoculated against the coronavirus, and the pandemic’s end finally seems to glimmer into view, scientists are envisioning what a postvaccine world might look like — and what they see is comforting.
The coronavirus is here to stay, but once most adults are immune — following natural infection or vaccination — the virus will be no more of a threat than the common cold, according to a study published in the journal Science on Tuesday and reported in the New York Times.
12/28/2021 The Science Behind How the Coronavirus Affects the Brain, WSJ Video
New research could help explain why thousands of Covid-19 survivors are facing debilitating neurological symptoms months after initially getting sick.
12/10/2020 Genomic Vaccines Fight Disease in Ways Not Possible Before. Rudy Giuliani was allocated one of the only 108 doses distributed to Washington D.C.
11/18/2020 How Doctors Can Predict Who Dies From COVID, Mike Hansen MD (a 7 minute youtube tutorial)
Mortality was 28.8% in the group that met criteria, vs 6.6% in those who did not meet criteria. So if they met cytokine storm criteria, their likelihood of dying was 4 times higher. And how accurate was this prediction model? Pretty accurate, as this study had a specificity of 79% and a sensitivity of 85%, which is a lot of predictive power.
11/9/2020 How the Coronavirus Hacks the Immune System, by James Somers, The New Yorker
At a laboratory in Manhattan, researchers have discovered how SARS-CoV-2 uses our defenses against us. TenOever’s team quickly discovered that sars-CoV-2 was uncannily good at disrupting cellular programming. A typical virus replaces less than one per cent of the software in the cells it infects. With sars-CoV-2, tenOever said, about sixty per cent of the RNA in an infected cell is of viral origin—“which is the highest I’ve ever seen. Polio comes close.” Among other things, the virus rewires the alarm system that cells use to warn others about infection.
11/5/2020: Clots, Strokes And Rashes. Is COVID-19 A Disease Of The Blood Vessels? by Will Stone, NPR
Some of the earliest insights into how COVID-19 can act like a vascular disease came from studying the aftermath of the most serious infections. Those reveal that the virus warps a critical piece of our vascular infrastructure: the single layer of cells lining the inside of every blood vessel, known as the endothelial cells or simply the endothelium.
Dr. William Li, a vascular biologist, compares this lining to a freshly resurfaced ice skating rink before a hockey game on which the players and pucks glide smoothly along.
"When the virus damages the inside of the blood vessel and shreds the lining, that's like the ice after a hockey game," says Li, a researcher and founder of the Angiogenesis Foundation. "You wind up with a situation that is really untenable for blood flow."
9/18/2020 Stroke patients with COVID-19 experience more severe symptoms, a much higher mortality rate, by Michael Walter, Cardiovascular Business
While the study did only focus on a limited number of patients, the authors also noted that the mortality rate was 44.4% for stroke patients with COVID-19 compared to 7.6% for those without COVID-19. For discharged patients, the average length of hospital stay was also longer if the patient had COVID-19.
8/13/2020: Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: a population-based cohort study, by Naomi Holman, PhD, Peter Knighton, MPhys, Prof Partha Kar, MD, Jackie O'Keefe, MSc, Matt Curley, BA, Andy Weaver, MSc, et al., The Lancet
Diabetes has been associated with increased COVID-19-related mortality, but the association between modifiable risk factors, including hyperglycaemia and obesity, and COVID-19-related mortality among people with diabetes is unclear. We assessed associations between risk factors and COVID-19-related mortality in people with type 1 and type 2 diabetes.
8/11/2020 Why the Heart Attack Death Rate Has Doubled During COVID-19, by Brian Krans, Healthline
5/29/2020: Medium: Coronavirus May Be a Blood Vessel Disease, Which Explains Everything, by Dana G. Smith
“It turns out that both statins and ACE inhibitors are extremely protective on vascular dysfunction,” Mehra says. “Most of their benefit in the continuum of cardiovascular illness — be it high blood pressure, be it stroke, be it heart attack, be it arrhythmia, be it heart failure — in any situation the mechanism by which they protect the cardiovascular system starts with their ability to stabilize the endothelial cells.”
Mehra continues, “What we’re saying is that maybe the best antiviral therapy is not actually an antiviral therapy. The best therapy might actually be a drug that stabilizes the vascular endothelial. We’re building a drastically different concept.”
5/21/2020: NEJM: Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19, by Maximilian Ackermann, M.D., Stijn E. Verleden, Ph.D., Mark Kuehnel, Ph.D., Axel Haverich, M.D., Tobias Welte, M.D., Florian Laenger, M.D., Arno Vanstapel, Ph.D., Christopher Werlein, M.D., Helge Stark, Ph.D., Alexandar Tzankov, M.D., William W. Li, M.D., Vincent W. Li, M.D., et al.m
The lungs from patients with Covid-19 also showed distinctive vascular features, consisting of severe endothelial injury associated with the presence of intracellular virus and disrupted cell membranes. Histologic analysis of pulmonary vessels in patients with Covid-19 showed widespread thrombosis with microangiopathy. Alveolar capillary microthrombi were 9 times as prevalent in patients with Covid-19 as in patients with influenza (P<0.001). In lungs from patients with Covid-19, the amount of new vessel growth — predominantly through a mechanism of intussusceptive angiogenesis — was 2.7 times as high as that in the lungs from patients with influenza (P<0.001).
5/18/2020: Medium: Every Covid-19 Symptom We Know About Right Now, From Head to Toe, by Robert Roy Britt
5/4/2020 Why Lying Face-Down Helps Relieve Coronavirus Symptoms, by Jesse Smith, 5/4/2020
How 'proning' Covid-19 patients helps them breathe
How Covid-19 Immunity Compares to Other Diseases
4/28/2020 COVID-19: What the data shows, Heart & Stroke
4/24/2020: Daily Beast: How the Coronavirus Sneaks into Your Body, A Rabbit Hole Deep Dive
In order to find which cells might be the gateways for the virus, Cambridge researchers turned to the Human Cell Atlas. The atlas, launched in 2016, acts as a kind of map for the hundreds of different kinds of cells in your body, their characteristics, the genes they contain, and their relationship to other cells.
The coronavirus works by attaching its spike protein to a particular receptor on the outside of human cells referred to as ACE2 and a protein in cell membranes named TMPRSS2 which primes those receptors for the virus to enter. The cells with the highest levels of ACE2 and TMPRSS2 turned out to be in the nose — goblet cells that make mucus and ciliated cells, tiny cells that look like miniature wheat fields which clean stray bits of snot and foreign organisms out of your airways.
While the highest levels of ACE2 and TMPRSS2 were found in cells in the nose, the Cambridge team also found high levels in cells associated with other organs. Cells in the human cornea and intestines also had plenty of the coronavirus-friendly proteins
At the outset of the pandemic, a pneumonia specialist in China became infected after inspecting a hospital while wearing an N95 mask and no eye protection and developed conjunctivitis shortly before becoming symptomatic.
4/23/2020: Nature Medicine: SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes, by Waradon Sungnak, Ni Huang, Christophe Bécavin, Marijn Berg, Rachel Queen, Monika Litvinukova, Carlos Talavera-López, Henrike Maatz, Daniel Reichart, Fotios Sampaziotis, Kaylee B. Worlock, Masahiro Yoshida, Josephine L. Barnes & HCA Lung Biological Network
We investigated SARS-CoV-2 potential tropism by surveying expression of viral entry-associated genes in single-cell RNA-sequencing data from multiple tissues from healthy human donors. We co-detected these transcripts in specific respiratory, corneal and intestinal epithelial cells, potentially explaining the high efficiency of SARS-CoV-2 transmission.
We provide our data in a comprehensive, open and user-friendly fashion at www.covid19cellatlas.org
4/20/2020: The Lancet: Endothelial cell infection and endotheliitis in COVID-19, by Zsuzsanna Varga, Andreas J Flammer, Peter Steifer, Martina Haberecker, Rea Andermatt, Annelies S. Zinkernagel, et al
4/17/2020: Science: How does coronavirus kill? Clinicians trace a ferocious rampage through the body, from brain to toes, by Meredith Wadman, Jennifer Couzin-Frankel, Jocelyn Kaiser, Catherine Matacic
How the virus attacks the heart and blood vessels is a mystery, but dozens of preprints and papers attest that such damage is common. A 25 March paper in JAMA Cardiology documented heart damage in nearly 20% of patients out of 416 hospitalized for COVID-19 in Wuhan, China. In another Wuhan study, 44% of 36 patients admitted to the ICU had arrhythmias.
The disruption seems to extend to the blood itself. Among 184 COVID-19 patients in a Dutch ICU, 38% had blood that clotted abnormally, and almost one-third already had clots, according to a 10 April paper in Thrombosis Research. Blood clots can break apart and land in the lungs, blocking vital arteries—a condition known as pulmonary embolism, which has reportedly killed COVID-19 patients. Clots from arteries can also lodge in the brain, causing stroke. Many patients have “dramatically” high levels of D-dimer, a byproduct of blood clots
4/11/2020: The Mercury News: When coronavirus kills, it’s like death by drowning — and doctors disagree on best treatment, by Lisa M. Krieger
In a comparison of very sick patients in China, shortness of breath began around the seventh day of their illness, with sepsis starting on the ninth or 10th day, followed by ARDS and then ICU admission on the 12th day, said Babik. The heart and kidneys showed injury on the 15th day. On the 17th day, secondary infections began to set in. Patients died, on average, on the 19th day.
Most worrisome: As the disease progresses, ventilators aren’t saving people. Despite our best efforts, COVID-19 illness is far more lethal than traditional ARDS, claiming not 40% of victims but 70% or even 80%.
Twitter: I don’t usually rant on social media. However, after a week of service in the ICU, I’d like to get a few things off my chest. #COVID19 (1/10) by Sanjum S. Sethi MD, MPH Click here to access the Twitter thread
1) This is a horrible, relentless, nasty disease in its severe form. If the patient is obese and/or has renal failure, the prognosis is extremely grim. They are NOT dying from comorbidities. They are dying from COVID -19.
2) When I say relentless; most patients make some improvements initially (days 4-6), but decompensate with a 2nd cytokine storm (as many have described). It is this 2nd decompensation that is deadly and that we need to prevent.
3) We are forced to share dialysis circuits given the high percentage of renal failure (these people had normal kidneys before!) Why isn’t there more press for this fact? We need more machines to manage our patients effectively.
4) This IS ARDS full stop. While certain pts may be phenotypically different and benefit from lower PEEP, others de recruit quickly. Different phenotypes should be treated as such. We are seeing more atypical presentations than usual because the volume is tremendous.
5) My interest is in thrombosis and there is a definite hypercoagulable state associated with this illness. Anticoagulation is all over the place at different centers, but there is no randomized data yet to guide any of it (working on it).
6) Every single ICU patient (barring QTc issues) got hydroxychloroquine and it doesn’t seem to have helped. Maybe it helps for prophylaxis or in mild disease, but doesn’t appear to do anything once in ICU. It is NOT a pancea and should not be given indiscriminately.
7) Listen to people who have been studying viruses and ARDS before all this began and will continue to investigate/clinically deal with it long after we have all moved on. #COVID19 #DrFauci
8) Be skeptical, but armchair conspiracy theories without any viable solutions are extremely disheartening. We are all in this together, help us generate the data that will answer those questions you are skeptical about and more importantly help our patients.
9) The rapid dissemination of materials, protocols, data is truly impressive. I feel like every intellect is pointed at one problem. Further, the support from people inside and outside of the hospital is truly overwhelming and much appreciated.
I have only glimpsed what this disease can do, so hats off to the leadership for their transparency and stewardship over the last 6 weeks. It is remarkable to witness the level of dedication of each individual trying to make a difference.
The Daily Beast: Here’s Where Coronavirus Hides in Your Body, by David Axe, 4/10/2020
“Active virus-replication in the upper respiratory tract puts the prospects of COVID-19 containment in perspective,” the scientists wrote.
Close observers of coronavirus studies hailed the German team’s work. There’s “huge news” in the Nature paper, David Ostrov, a professor in the Department of Pathology, Immunology and Laboratory Medicine at the University of Florida College of Medicine, told The Daily Beast.
SARS-CoV-2 starts replicating in the throat, not the lungs. For that reason, a simple throat swab is enough to test for the virus. There’s probably no need for an intrusive, unpleasant nasal swab.
There’s bad news in the German study, too.
The antibodies our bodies produce in response to COVID-19 infection don’t actually destroy this virus. In that way, it is a lot like HIV.
The antibodies are not effective at clearing the virus,” Ostrov told The Daily Beast. “This is relevant when thinking about viruses and vaccines. HIV also stimulates production of antibodies that fail to clear the virus, as do many other viruses, such as hepatitis virus C.”
“People have tried and failed to generate vaccines against such viruses, so we should not be overconfident that a vaccine strategy will work,” Ostrov added.
The Washington Post: I spent six days on a ventilator with covid-19. It saved me, but my life is not the same. By David Lat, 4/9/2020
I spent my first few days in the hospital in stable condition, receiving supplemental oxygen. But on the evening of March 20, I took a turn for the worse. Late that night, I learned that I would need to be intubated, or placed on a ventilator.
This terrified me. A few days earlier, after my admission to the hospital, my physician father had warned me: “You better not get put on a ventilator. People don’t come back from that.”
As a patient whose life was saved by a ventilator, I believe it is an outrage and an embarrassment that a nation as wealthy as ours is even discussing possible ventilator shortages. Thankfully the United States has managed to avoid widespread rationing partly due to ventilators being sent from places of low need to places of high need. We need to make sure that every patient who needs a ventilator can get one so that as many of them as possible can survive.
This is especially true because survival rates of ventilated patients are low. My father’s dark comment reflected a grim reality: 40 percent to 50 percent of patients with severe respiratory distress do not survive being on ventilators. In New York City, where I was hospitalized, 80 percent or more of coronavirus patients who end up on ventilators have died.
SciTechDaily: Possible Coronavirus Treatment? Head Lice Drug Ivermectin Is Being Tested, By Andrew McLachlan, the Head of School and Dean of Pharmacy, University of Sydney, Australia, 4/6/2020
SciTechDaily: Coronavirus Fight: Scientists Identify COVID-19 Drug That “Kills” the Virus Within 48 Hours, Wagstaff et al, 4/5/2020
Ivermectin is an FDA-approved anti-parasitic drug that has also been shown to be effective in vitro against a broad range of viruses including HIV, Dengue, Influenza and Zika virus.
While shown to be effective in the lab environment, Ivermectin cannot be used in humans for COVID-19 until further testing and clinical trials have been completed to confirm the effectiveness of the drug at levels safe for human dosing.
The wholesale cost in the developing world for the tablets is about US $0.12 for a course of treatment. In the United States, the costs is less than US$50.
So, the drug would be only 400x as expensive here, half of that plundered by Health Insurance Industrial Complex parasites.
Antiviral Research: The FDA-approved Drug Ivermectin inhibits the replication of SARS-CoV-2 in vitro, by Caly, Druce, Catton, Jans, & Wagstaff, 4/3/2020
AAPS Journal, The Pharmacokinetics and Interactions of Ivermectin in Humans—A Mini-review, by González Canga, A., et al, 1/25/2008
Although the efficacy of ivermectin has been established in humans against several parasite diseases, the pharmacokinetic properties of this compound are less well known in humans compared to animals. Potential drug-drug interactions and drug-food interactions exist for ivermectin, which should be considered during therapeutic use of this drug.
The New Yorker: The Quest for a Pandemic Pill, by Matthew Hutson, 4/6/2020
The New Yorker: How Does the Coronavirus Behave Inside a Patient?, by Siddhartha Mukherjee, 3/26/2020
Mukherjee's "The Emperor of All Maladies" won a Pulitzer Prize.
Los Angeles Times: Coronavirus kills some people and hardly affects others: How is that possible? by Deborah Netburn, 4/4/2020
CNN: Experts tell White House coronavirus can spread through talking or even just breathing, By Elizabeth Cohen,4/2/2020
Medium: NYC Lung Doctor Tells His Family How to Protect Themselves from COVID-19, by Paul Anderson, 3/27/2020
The New Yorker: From Bats to Human Lungs, the Evolution of a Coronavirus, by Carolyn Kormann, 3/27/2020
Since January, nearly eight hundred papers about the virus have been posted on BIORxiv, a preprint server for studies that have not yet been peer-reviewed. More than a thousand coronavirus genome sequences, from different cases around the world, have been shared in public databases. “It’s insane,” Kristian Andersen, a professor in the Department of Immunology and Microbiology at Scripps Research, told me. “Almost the entire scientific field is focussed on this virus now. We’re talking about a warlike situation.”
Medium: This Is How Your Immune System Reacts to Coronavirus, by Dana G Smith, 3/24/2020
Youtube: Ninja Nerd: Epidemics and the coronavirus infection, the ARDS and pneumonia timeline explained. 3/16/2020
Youtube: Ninja Nerd: COVID-19 | Corona Virus: Treatment, Prognosis, Precautions, 3/18/2020
Youtube: Duc C. Vuong, MD, explains how COVID-19 kills and why you can't be saved, 3/23/2020
CNN: Video reveals lung damage in US coronavirus patient: 'People need to take this seriously' By Brian Fung and Jen Christensen, 3/27/2020
University of Texas: COVID-19 Can Cause Cardiac Injury – Even in Patients Without Underlying Heart Conditions, University of Texas Health Science Center at Houston, 3/27/2020
In a clinical bulletin issued by the American College of Cardiology, it was revealed that the case fatality rate of COVID-19 for patients with cardiovascular disease was 10.5%. Data also points to a greater likelihood that individuals over the age of 65 with coronary heart disease or hypertension can contract the illness, as well experience more severe symptoms that will require critical care.
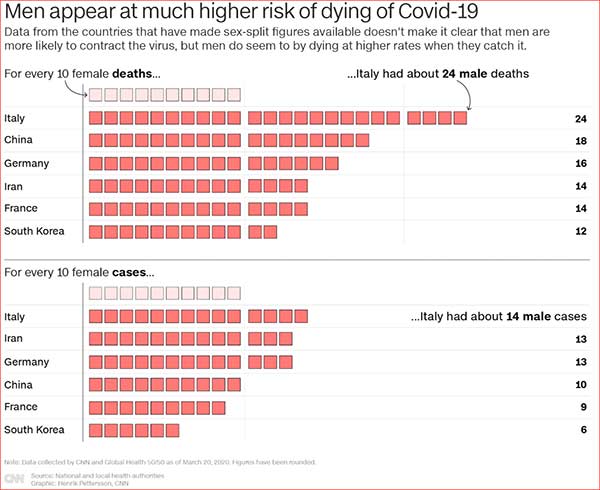
CNN: Here's why the coronavirus may be killing more men than women. The US should take note, By Katie Polglase, Gianluca Mezzofiore and Max Foster, 3/24/2020
Cell: Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein, Alexandra C. Walls, Young-Jun Park, M. Alejandra Tortorici, Abigail Wall, Andrew T. McGuire, David Veesler, 3/9/2020
Highlights
- SARS-CoV-2 uses ACE2 to enter target cells
- SARS-CoV-2 and SARS-CoV bind with similar affinities to ACE2
- Structures of SARS-CoV-2 spike glycoprotein in two conformations
- SARS-CoV polyclonal antibodies inhibit SARS-CoV-2 spike-mediated entry into cells
Time: About Dr. Frederick Murphy, the first CDC Virologist to image the Ebola Virus, Alexandra Sifferlin, 10/13/2014
Time: SARS, Ebola, Marburg, MERS infection rate and death tolls compared, David Johnson, 2014/10/13
Harvard Gazette: Samples from those who had COVID-19 could illuminate true infection rate, lethality, vaccines, Stephanie Dutchen, 3/25/2020
VirScan promises to help Elledge and colleagues identify which parts of the virus the immune system responds to.
Recent work from his group suggests that people all over world infected with a particular virus make antibodies against the same proteins — “even the same amino acids” — on that virus, Elledge said.
That’s surprising, considering how many epitopes viruses have and how many antibodies are in the body’s arsenal, said Elledge. The findings led him to suspect that some epitopes are, in effect, decoys, and therefore, that not all antibodies have the desired neutralizing effect.
“The immune system may be sending out all these antibodies like shooting a shotgun and hoping some of the spray will hit the target, neutralizing some critical part of the virus,” he said.
In principle, said Elledge, VirScan could indicate which epitopes are useful targets against the new coronavirus and which are just noise. Then researchers could eliminate the useless ones from vaccines they’re developing.
1918 Spanish Flu historical documentary | Swine Flu Pandemic | Deadly plague of 1918, 10/2/2018
Cambridge University: Spanish Flu: a warning from history, 11/30/2018
6/26/2017 Genomic Vaccines Fight Disease in Ways Not Possible Before, by Geoffrey Ling, Scientific American
Vaccines composed of DNA or RNA, instead of protein, could enable rapid development of preventives for infectious diseases
- You are here:
-
Home

- hidden covid 19